

Fire or Ice?
Although this may seem trivial to some, the number of patients that are unaware of whether to apply hot or cold therapy to an area has prompted me to write this article.
Let’s start with a common scenario… A player feels a sudden sharp pain in the hamstrings whilst playing soccer. He finds it difficult to continue playing. Should he use ice or a hot water bottle?
The second scenario…. A few days after a heavy workout, a player feels strong discomfort in the hamstrings when walking or climbing stairs. What should he do??
Both these scenarios involve a muscular issue involving the hamstrings, however they should be handled very differently. To understand why, we need to understand the effects of heat and ice…
Heat:
- Increases blood flow to the area through dilating blood vessels, thus transporting proteins, nutrients, and oxygen for better healing
- Increases cell metabolism
- Increases the tissues ability to stretch (extensibility)
- Relieves muscular spasm
Cold:
- Reduces blood flow through constricting vessels, thus reducing internal bleeding
- Decreases cell metabolism which will slow down an inflammatory reaction
- Reduces pain (analgesia)

So, in cases of ACUTE INJURIES (where we are trying to reduce the inflammatory response), one should apply ICE to the area as soon as possible and continue for the first 72 hours. It is recommended to only apply ice for 10 minutes and then wait 50minutes before applying again (i.e. 10 minutes every hour). This is to prevent a reaction (known as the “Hunting response”) which will actually INCREASE blood flow to an area that gets too cold for too long.

On the other hand, HEAT is used to treat CHRONIC INJURIES where there is no swelling or bruising. Usually this is for sore, nagging muscular aches or stiff joints. It’s great for muscular tension and can be applied for 15-20 minutes at a time, taking care not to burn the skin. This can be in the form of a hot water bottle/heat packs or just a really hot bath.
So from the above it should be obvious that scenario number 1 needs to ICE his injury as he probably has a hamstrings muscle tear. He should also follow the PRICER principles – see this article
The athlete in scenario 2 should use HEAT and stretching to relieve his muscular pain as his is not an acute injury and most likely post training muscle stiffness (delayed onset muscle soreness – DOMS).
Hope that this helps you clear up when to apply which therapy.
Ric@PhysioPRO
BY: Riccardo Vaccaro
General Health/Fitness

The Important Role of Fascia
As physiotherapists we often deal with a lot of myofascial problems. Most people understand the first part of this word i.e. Myo-referring to the muscular system but I want to explain the second component of this word a little better – Fascia – and its relevance to how your body functions.
Firstly – what is Fascia?
Fascia is a slightly mobile connective tissue spread throughout the body in a three dimensional web. It surrounds every muscle, every fascicle, every fibril (fibre) and every microfibril that make up your muscles. It mainly consists of collagen and elastin.

Think of your body’s fascial system as a multi-layered body stocking, with fascial sheaths wrapping the muscles and weaving in layers throughout the body. Because of this, stress in any area of the body has an effect on every other part of the body. The Fascia basically connects everything!
What does the Fascia do?
Fascia plays an important role in supporting, stabilizing and protecting the structures it surrounds. In other words, it provides postural balance. The Fascial system conveys mechanical information via tension and compression and has a role in cellular nutrition. The deep fascia also provides a surface area for muscles attachment.
In its optimal condition, fascia is a loose, moist tissue. When there is continual loose movement and balance in the body, the fascial body stocking stays loose and mobile, facilitating movement between different parts of the body.
However, under continual stress (caused by poor postures and mechanical forces exerting abnormal tension on muscles) as well as lack of movement, fascia becomes rigid and loses its fluidity causing muscle undernourishment. Layers of fascia begin to stick to one another, causing the “knots” you may have experienced in your muscles (trigger points). The sheaths of fascia stick in a systematic way, based on your habitual patterns of movement, or for some, lack of movement.
Therefore Myofascial release aims to reverse myofascial deformation and re-open the tissue to increase the fluid flow to affected areas (restore the viscosity of the tissue), muscle function and improve motor and sensory input. It is also very important to decrease the abnormal pull (stress) on the myofascia to correct altered joint alignments.
As you can see the fascial system plays a major role in muscular injuries and pain and if overlooked by your therapist could contribute to recurring and prolonged aches and pains.
Andrew@PhysioPRO
BY:
Back injuries / General Health/Fitness / Neck injuries

Resistance Training
As a physio, I often hear these questions:
• “What type of exercise should I be doing to build muscle?
• “I’m going to gym and training hard…but I don’t see the results on the sports field. What am I doing wrong?”
Here’s some food for thought:
In order to obtain maximum muscle growth and see rapid progress it is important to bring  variety into your training and put your body through different kinds of resistance exercises. Body- weight training – working against your own weight – is a great way to train as it does not require any equipment and all of the muscles of the body can be worked. Unfortunately when a lot of people start out, many of them are unable to do pull-ups or push-ups lifting their entire body weight. So it is easier to start
variety into your training and put your body through different kinds of resistance exercises. Body- weight training – working against your own weight – is a great way to train as it does not require any equipment and all of the muscles of the body can be worked. Unfortunately when a lot of people start out, many of them are unable to do pull-ups or push-ups lifting their entire body weight. So it is easier to start  with additional resistance training i.e. using dumbbells or handheld weights. Dumbbells are an extension of body-weight training, but are less restrictive as you can vary the resistance slowly as you get stronger. Stronger athletes can go beyond using only their body weight by increasing the weight of the dumbbells.
with additional resistance training i.e. using dumbbells or handheld weights. Dumbbells are an extension of body-weight training, but are less restrictive as you can vary the resistance slowly as you get stronger. Stronger athletes can go beyond using only their body weight by increasing the weight of the dumbbells.
Elastic Resistance – using the resistance of an elastic band – is also a great way to train as the elastic band provides significant resistance but does not weigh anything (plus they are easy to transport and store at home).
Elastic resistance is very different to the resistance provided by body-weight or dumbbells. The more you pull on an elastic band the greater the resistance, so there will be more resistance at the end (inner range) of the movement.It is very important to maintain control throughout the entire movement – while pulling in and while letting go – and not just let the elastic recoil rapidly back to the starting position at the end of the repetition.
 An important type of resistance – especially for athletes – and one that people don’t focus on much is Plyometric Resistance. Plyometrics bring together the strength gained in the gym and the increase in performance gained by high intensity exercise. It is particularly important for athletes who need muscle reactivity, and can help you transform your strength into explosiveness which is essential on the sports field! Plyometric resistance comes into play when you force your muscles to abruptly stop a movement and then go in the opposite direction e.g. jumping off a box, landing while absorbing the shock, and using it to jump as high and as fast as possible. Very, very important in any plyometric exercise is to limit contact with the floor, movements needs to be fast and explosive!
An important type of resistance – especially for athletes – and one that people don’t focus on much is Plyometric Resistance. Plyometrics bring together the strength gained in the gym and the increase in performance gained by high intensity exercise. It is particularly important for athletes who need muscle reactivity, and can help you transform your strength into explosiveness which is essential on the sports field! Plyometric resistance comes into play when you force your muscles to abruptly stop a movement and then go in the opposite direction e.g. jumping off a box, landing while absorbing the shock, and using it to jump as high and as fast as possible. Very, very important in any plyometric exercise is to limit contact with the floor, movements needs to be fast and explosive!
Too much of a good thing can very easily become a bad thing….same goes for plyometrics. So as soon as you notice that the time of contact with the floor becomes too long and you are slowing down too much, know that you are fatiguing and the set should be interrupted for a slight rest time.
In conclusion, it would not be wise to choose one type of resistance over another but rather to combine all of them into your training routine. The net effect will be putting your body through cumulative resistance training that is superior to a focus only on any one particular method of training.
Happy training 🙂
Andrew@PhysioPRO
BY:
General Health/Fitness

First Aid CPR “HARD and FAST”
While not typically physiotherapy-related I thought it important to write on something everybody should know a little bit about – First Aid.
First Aid refers to emergency assistance given to an injured or ill person using readily available materials. This aid ranges from something as basic as removing a splinter from a child’s finger and putting on a plaster on the wound to giving care to casualties of a motor vehicle accident and handing them over to a medical team.
As you can imagine this is a broad area to cover. This article will touch on the basics of First Aid administered on an unconscious adult patient. Overall, I strongly recommend attending a First Aid course as you never know when this key knowledge could help to save a life!
First Aid always aims to:
- Preserve life
- Prevent the illness or injury from becoming worse
- Promote recovery
If in a situation where a patient is unconscious the first thing to do is quickly assess the area for any hazards. You will be no help to the person if you rush into a potentially risky scenario and injure yourself in the process adding to the casualty count. Once the area is safe ascertain the patient’s unresponsiveness by talking to them – (ask and say ‘Hello?’) and then ask for assistance (call loudly for ‘Help’) to get someone to contact the emergency services. The sooner you get the patient medical attention the better! When deciding between calling an ambulance and transporting the patient yourself to the hospital, remember to ALWAYS preferably call an ambulance if you can. An ambulance is well equipped and the patient benefits from immediate medical help when trained paramedics arrive.
Administering CPR (Cardio-Pulmonary resuscitation):
While waiting for the ambulance, if an adult has collapsed and is unresponsive take 5 to 10 seconds to feel for a pulse. This is done by placing two fingers on the patient’s carotid pulse where we feel for the artery found just below the angle of the jaw.
If no pulse is felt ask a fellow bystander to contact the emergency services while you begin CPR as follows:
- Begin with chest compressions over the middle to lower half of the sternum (breast-bone).
- Interlock your fingers and keep your elbows locked straight.
- Press HARD and FAST.
- You must press the chest down at least 5cm with each compression.
- Remember to allow the chest to recoil between compressions.
- Compress at a rate of at least 100 compressions per minute (believe it or not, this rhythm corresponds nicely with the beat of the Beegees’ hit “ Staying Alive”… I can hear you tapping your feet!)
- If you have a barrier device available (mask or one-way protective valve to protect you from blood and air-borne pathogens) you can interrupt compressions to give 2 breaths after every 30 compressions. When giving breaths ensure that you see the chest rise with each breath you give. If no barrier device is available it is acceptable to provide “hands-only” CPR – unless you are comfortable providing mouth to mouth breathing to the victim.
Automated Electronic Defibrillators
Many public places such as gyms and airports have access to Automated Electrical Defibrillators (AED’s). Always call for one of these to be brought to a victim of cardiac arrest as soon as possible. Do not be frightened of using such a device as it is voice prompted and very user friendly. Once an AED has arrived turn it on and attach the pads to the victim by following the voice prompts. Always minimize interruptions to your chest compressions even when applying the AED. Follow the instructions of the AED.
The AED will analyze the patient’s heart and will do one of two things:
1: Recommend a shock – if a shock is required the AED will advise to keep clear of the patient and direct you to press a button to give the patient a shock. After the shock has been administered you must immediately continue CPR, starting with chest compressions.
2: No shock advised – If the AED does not recommend administration of a shock immediately continue with chest compressions until the AED commands “Re-analyze”
When contacting emergency services for a patient undergoing CPR make sure to be as specific as possible about the scenario and let the emergency services know that CPR is underway. This will help prioritise your call at the dispatch office/call centre.
Key points:
Early activation of emergency services, good quality CPR (push HARD, push FAST) and early access to an AED.
If the victim resumes breathing and has a pulse place them on their side in what is called ‘the recovery position’. If they don’t resume breathing continue CPR until medical help arrives.
Useful First Aid courses are regularly held by the St John’s Ambulance Service and the academy of advanced life support {www.stjohn.org.za}
Emergency Services contact numbers: Netcare911 (082-911), ER24(084-124), Gauteng EMS (10177) or dial 112 or 911 from any cellphone.
CPR saves lives.
If you don’t believe me ask Vinny Jones. Watch www.youtube.com/watch?v=JR0aZX1_TD8 and remember ‘push hard and fast to ‘Staying Alive’!’
BY:
General Health/Fitness

Total Hip Replacements
A Total Hip Replacement – or THR as we like to call it in this business – is a surgical procedure in which diseased cartilage and bone, located at the head of the femur and acetabular cap, are replaced with artificial materials (a prosthesis).

More often than not, this is an elective procedure. Therefore, many older patients come to me for advice on whether or not to go for a THR. What I always tell them is that as with any surgical procedure there are potential risks, so it should not be entered into lightly and should be seen as a last resort. In my opinion, the biggest factor is how the operation will affect quality of life. If one’s current hip condition is impairing function to a significant extent – such that quality of life is severely diminished – then a THR would be of great benefit.
Who needs a THR?
- Patients with severe Osteoarthritis
- Patients who have tumours in the hip that have destroyed the hip joint rendering it dysfunctional
- In cases of avascular necrosis (hip joint is destroyed due to lack of blood supply) can develop due to fractures, drug and alcohol abuse and other diseases.
- Patients with intense chronic pain persists despite the use of anti-inflammatories for more than 6 months, adversely affecting sleep, ability to work and movement.
A THR is not recommended for patients with:
- A current hip infection
- Paralysis of quadriceps
- Severe blood disease
- Nerve disease affecting the hip
- Severe mental dysfunction
- Morbid obesity i.e. weighing more than 140kg
If possible, once one has decided to have the operation, it would be of great benefit to start pre-operative strengthening exercises to assist with rehabilitation post-surgery.
To prevent post operative risks, rehabilitation starts immediately after the operation. This includes circulatory and isometric exercises. On Day 1 post-surgery patients are usually sitting up, out of bed and working on strengthening the quadriceps. By Day 2 patients are walking with an assistive device (normally a walker). Physiotherapy is critical in the coming months to regain strength and functional activity.
For the first 3 months post-surgery it’s prohibited to lie on one’s side or cross one’s legs as the hip could dislocate in these positions. After 6 months normal daily activities should continue comfortably.
Always remember to inform your health care professionals that you have had a THR and avoid strenuous activities, running, contact sports etc as this will decrease the life span of your THR. Swimming is a very good way to strengthen and increase the mobility of your hip without causing too much strain on and friction at the joint.
Andrew Savvides
PhysioPRO
BY:
General Health/Fitness / Hip injuries / Lower Limb injuries

Don’t just POP that PILL!
Having repeated this bit of info over and over again to a lot of my patients, I decided its time to put it in writing….
Lets me just start off by saying, Anti-Inflammatories are over-prescribed! At the first sign of any pain or swelling, a doctor will usually pull out his/her referral pad and write a script for anti-inflammatories without giving it a second thought. DON’T POP THOSE PILLS!
Worldwide, 73 000 000 prescriptions of Nonsteroidal anti-inflammatory drugs (NSAIDs) are written yearly. Although theses drugs are very useful at relieving pain, decreasing inflammation, decreasing elevated body temperature, and decreasing blood clotting they are also associated with frequent and significant side effects.
The two main problems with the prescribing of NSAIDs are (1) the TIMING of use and (2) the RELEVANCE to the tissue/injury being treated.
(1) Taking NSAIDs during the acute stage of an injury (usually 48-72hrs) is usually not recommended as this STOPS the inflammatory process. Inflammation is the first key step to tissue healing, so by STOPPING this phase, you are delaying the tissue healing process. Rather LIMIT this phase using the PRICE principles (see our previous article “Acute Injury Management”). Taking NSAIDs in the later (regenerative) phase of healing has also been shown to impede regeneration and increase fibrosis in tissue.
That said there is a narrow window period (the sub-acute phase) where NSAIDs could be used. This is usually 72hrs-10days post injury, but could vary depending on the injury and person.
(2) Understanding the injury/pathology- Of considerable importance to us in the Sports Medicine field are the side effects related to impaired healing in ligaments and bones. Ligament injuries treated with NSAIDs in the acute phase have been shown to have up to a 32% decrease in tensile strength, and fractures have been shown to be 5 times more likely not to unite following NSAID use!! But your doctor gave you NSAIDs for that ankle sprain right???
Tendinopathies (like Achilles tendinopathy, Tennis Elbow etc.) are not inflammatory conditions, so the prescribing of NSAIDs in these cases are useless and can only have negative side-effects. Acute muscle tears are another instance where one should rather avoid NSAID’s as they have been shown to delay healing. However, chronic inflammatory conditions like Rheumatoid Arthritis and Tenosynovitis (inflammation of the tendon sheath) do benefit from NSAID use.
So what’s the take home message?
NSAIDs are effective, but their application to specific tissues and injuries are complex, so don’t rush off to the pharmacy and buy them without first consulting your Sports Physio or Physician.
If you do have a musculoskeletal injury, first take Paracetomol (as found in Panado), as it is effective in relieving pain but without the side effects on tissue healing.
If you are not sure, avoid NSAIDs for the first 3 days post injury and don’t take them for more than 7 days without consulting a health professional.
Ric@PhysioPRO
BY: Riccardo Vaccaro
General Health/Fitness

The trouble with being immobile
Our bodies were designed to move and participate in the different activities of daily living. So what happens when we, recovering from an injury or illness, find ourselves restricted to bed rest for a prolonged period of time? The way in which immobility affects our body and what we can do to prevent the associated complications, is worth exploring further.
Effect on the Cardiovascular system (heart and blood vessels)
Any activity of the muscles will push blood through your body. This blood flow through your veins and back to your heart will increase your circulation. So, when you are just lying in bed and not using those muscles, one risks peripheral oedema – swelling of your hands and feet.
Furthermore, being immobile for prolonged periods will see your resting heart rate increase as the heart needs to work harder to pump the blood through your body, without help from the body’s natural movement and muscle contractions. There will also be a decrease in the ability of the blood to take up oxygen, which can cause you to become dizzy or faint especially when u stand up after prolonged bed rest (postural hypotension).
Deep Vein Thrombosis is a serious complication associated with immobilisation. Which occurs due to an increase in the viscosity(thickening) and slowing down of the blood which basically forms a clot in the vessel. Dislodgement of a venous clot that lodges itself in the lung tissue is called a Pulmonary Embolism and may be fatal.
Effect on the Respiratory System
We all have fine little hairs in the airways that sweep secretions like mucous, phlegm etc upward and out of our respiratory systems. But immobilisation reduces the action of these cilia, or little hairs, and this inability to clear secretions may lead to infections such as pneumonia
Lung collapse (Atelectasis) – especially in the basal lobes of the lung – can also result as respiratory secretions accumulate in these lower lobes in the gravity dependent position and cause the small airways to close.
Effect on the Metabolic system
Prolonged bed rest causes the bones to lose calcium and potassium, as oesteoblastic activity(bone development) is reduced due to the lack of weight going throught the bones. This causes a decrease in the bone integrity or density of the bone matrix perhaps resulting in osteoporosis.
One may also develop kidney stones due to pooling of urine in the kidneys and bladder.
Effect on the Musculoskeletal system
It’s pretty obvious that if you not using your muscles that they will atrophy and weaken. Joint contractures – restrictions in the normal range of motion caused by peri-articular and intra-articular connective tissue – can occur. Basically your joints get stuck!
Another major complication of immobility is the possible development of pressure sores. These develop due to unrelieved pressure especially over areas where the skin lies close to bone. Pressure sores cause tissue death (necrosis). Once developed, these sores take a long time to heal and can be a source of secondary infection in the body.
Effect on the mind
To add to all these negative physical as well as physiological complications, being immobile affects one emotionally. People may have increased anxiety and depression and a decreased attention span.
What can you do?
Nearly all of these complications can be prevented with the right exercises and with help from your physiotherapist.
Undertake active circulatory exercises often, during the day, including foot pumping, static quadriceps and gluteal contractions, and active hip and knee exercises. These will all help to increase your circulation and benefit your cardiovascular system.
To deal with any respiratory problems work on increasing the efficiency of the lungs through deep breathing exercises and physiotherapy to the chest.
Weight bearing exercises are essential to prevent weakening of bones. Start getting out of bed and being mobile as soon as possible. While immobile, undertake exercise programmes that offer resistance training, either with your physiotherapist or using free weights.
As much active movement as possible should be facilitated, to make sure your muscles don’t weaken and shorten, always ensuring that the exercise is carried out to include its full range of motion to prevent contractures.
Ensure pressure relief, particularly on areas where the skin lies close to bone, by changing position every 2 hours, to prevent pressure sores and secondary infection.
It is also very important to try stay positive and motivated in this time of immobility. Speak to people, family, friends even your health care professionals. Set goals for yourself and your recovery and achieve them.
Until next time…Stay ACTIVE!
Andrew Savvides
PhysioPRO
BY:
General Health/Fitness

Healing Heels….
Having had an unusual number of patients at my practice with this condition, I decided to tell you a little more on Plantar Fasciitis…
Plantar Fasciitis (PF) is a painful and often prolonged injury. The source of the pain is a thick “band” under the foot, connecting the heel bone (calcaneus) to the toes, which becomes inflamed. It is usually associated with morning pain (first few steps) felt under the heel. Pain is usually also present following sitting or standing too long, climbing stairs or after exercise.
Some of the risk factors include very high or very flat foot arches, wearing shoes that are not supportive of the arch, sudden increase in weight and unaccustomed exercises. Having tight Achilles tendons and calf muscles have also been shown to increase the risk of this injury, hence ladies that wear high heels a lot are prone to developing it.
So I had to ask my self why the sudden increase in this condition lately? Well it turns out most of my patients started feeling pain from the change of winter to summer. They went from supportive boots or closed shoes to wearing flip-flops with absolutely no arch support, almost overnight. This lead to stretching and irritation of the band, and hence the start of PF.
Treatment modalities that have proven effective are:
- Soft tissue release and stretching of the calf complex (see stretches as per “A real pain in the calves“)
- Stretching the plantar fascia (by rolling a golf ball under the arch)
- Icing under the foot to relieve pain
- Strapping to support the arch
- Using a gel heel cup to alleviate pressure
I have found that dry needling the plantar fascia reduces pain, and I also recommend that most of my patients avoid wearing flat, unsupportive shoes. A good trick to stretch the band and relieve pain at the same time is to freeze a bottle of water and then use this cold, hard bottle by rolling it quite hard underneath the arch.
Im not quite sure why, but doctors still send patients with PF for x-rays to look for something called a “heel spur”? Having this spur is not a diagnostic feature (i.e. you could have the spur and NOT have PF) and surgery to remove this bone formation is rarely necessary.
As mentioned, the condition can sometimes take up to a year to heal, so don’t prolong your pain, come see your physiotherapist.
Ric@PhysioPRO
BY: Riccardo Vaccaro
Foot injuries / Lower Limb injuries
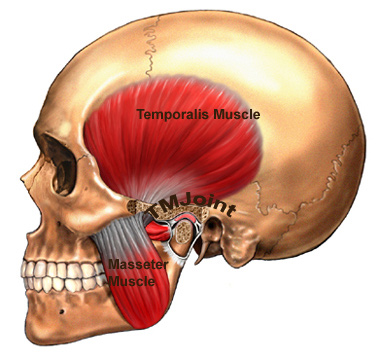
The TMJ- the little joint with a large role
The Temporomandibular joint (TMJ) is a little joint with a big name and even larger role to play in day to day life. It’s found between the jaw bone and one of the bones in the skull – just below the temples.

When one considers how much we use this joint in daily activities it isn’t very surprising that this joint is subject to wear and tear. This, because it’s involved in chewing and talking (ceaseless activities for some). The TMJ can even be damaged while a person sleeps, as clenching or grinding one’s teeth will cause the joint’s cartilage lining to wear away.
Common causes of TMJ dysfunction are:
- Poor posture i.e. one that sees the chin poke out
- Habitual or excessive chewing of gum
- Previous trauma to the area
- Dental problems
- Stress and clenching of teeth
TMJ dysfunction could see people experience limited motion and a general dull ache over the side of the face as well as local muscle tenderness. A ‘click’ may also be present as patients open and close their mouth, as the joint dislocates and relocates back into place. Headaches, sinus and neck problems can all be associated with TMJ dysfunction. It’s clearly a very important joint to keep clear of damage.
A quick self test for TMJ health:
- Place 3 fingers vertically into your mouth. Inability to do this indicates TMJ hypomobility.
Using physiotherapy to treat damage to the TMJ involves:
- myofascial release
- massage
- gentle stretches
- accessory mobilizations
- electrotherapy
- postural correction
- re-education.
Most important is identifying and addressing the cause of the dysfunction.
So if you think you are having problems in this particular area, do not fear. Help is always at hand. Visit your PhysioPRO practice for an assessment.
Until next time…Keep Smiling 🙂 and chewing and talking.
Andrew Savvides
PhysioPRO
BY:
General Health/Fitness / Neck injuries