

The Important Role of Fascia
As physiotherapists we often deal with a lot of myofascial problems. Most people understand the first part of this word i.e. Myo-referring to the muscular system but I want to explain the second component of this word a little better – Fascia – and its relevance to how your body functions.
Firstly – what is Fascia?
Fascia is a slightly mobile connective tissue spread throughout the body in a three dimensional web. It surrounds every muscle, every fascicle, every fibril (fibre) and every microfibril that make up your muscles. It mainly consists of collagen and elastin.

Think of your body’s fascial system as a multi-layered body stocking, with fascial sheaths wrapping the muscles and weaving in layers throughout the body. Because of this, stress in any area of the body has an effect on every other part of the body. The Fascia basically connects everything!
What does the Fascia do?
Fascia plays an important role in supporting, stabilizing and protecting the structures it surrounds. In other words, it provides postural balance. The Fascial system conveys mechanical information via tension and compression and has a role in cellular nutrition. The deep fascia also provides a surface area for muscles attachment.
In its optimal condition, fascia is a loose, moist tissue. When there is continual loose movement and balance in the body, the fascial body stocking stays loose and mobile, facilitating movement between different parts of the body.
However, under continual stress (caused by poor postures and mechanical forces exerting abnormal tension on muscles) as well as lack of movement, fascia becomes rigid and loses its fluidity causing muscle undernourishment. Layers of fascia begin to stick to one another, causing the “knots” you may have experienced in your muscles (trigger points). The sheaths of fascia stick in a systematic way, based on your habitual patterns of movement, or for some, lack of movement.
Therefore Myofascial release aims to reverse myofascial deformation and re-open the tissue to increase the fluid flow to affected areas (restore the viscosity of the tissue), muscle function and improve motor and sensory input. It is also very important to decrease the abnormal pull (stress) on the myofascia to correct altered joint alignments.
As you can see the fascial system plays a major role in muscular injuries and pain and if overlooked by your therapist could contribute to recurring and prolonged aches and pains.
Andrew@PhysioPRO
BY:
Back injuries / General Health/Fitness / Neck injuries

Preventing Poor Posture
So as promised, following my last article “Sitting posture and (D)evolution of man”, here are a few stretches that you can do at your office or home to help loosen up those stiff muscles affected by poor sitting posture.
Please note that these are general stretches for people without neck or lower back pain. If you are already suffering from pain, you should rather consult your physio before attempting any of these stretches.
 1)Neck Retractions- Whilst sitting upright, try bringing your chin in, towards your neck.
1)Neck Retractions- Whilst sitting upright, try bringing your chin in, towards your neck.
You want to imagine that you are trying to make the back of your neck get longer (as if someone is pulling you up by your hair), whilst still looking forwards. If you are tight, you may feel a stretch at the base of your skull. Hold 10 seconds and repeat 10 times
 2) Neck flexion stretch- First retract your neck as shown above. Then, whilst still holding your chin tucked in, grab the top of your head using both hands and gently pull down.
2) Neck flexion stretch- First retract your neck as shown above. Then, whilst still holding your chin tucked in, grab the top of your head using both hands and gently pull down.
If done correctly, you should feel the whole back of your neck getting stretched. Hold 30 seconds and repeat 2-3 times.
 3) Seated rotations- Whilst sitting, turn to your right. Use your right arm to grab the back of the chair. Place your left hand on your right knee and then gently pull. Hold 30 seconds and repeat to the other side
3) Seated rotations- Whilst sitting, turn to your right. Use your right arm to grab the back of the chair. Place your left hand on your right knee and then gently pull. Hold 30 seconds and repeat to the other side
 4) Seated back extensions- Interlock your fingers behind your head. With your elbows pointing upwards, towards the ceiling, extend your upper back and try push your elbows further back. Hold 30 seconds and repeat 5 times.
4) Seated back extensions- Interlock your fingers behind your head. With your elbows pointing upwards, towards the ceiling, extend your upper back and try push your elbows further back. Hold 30 seconds and repeat 5 times.
 5) Side stretch-This stretch targets those tight muscles on the side of your neck (scaleni and upper fibres of trapezius) where most of us feel “knots”.
5) Side stretch-This stretch targets those tight muscles on the side of your neck (scaleni and upper fibres of trapezius) where most of us feel “knots”.
Whilst sitting, grab the seat of the chair with your left hand (this stops your left shoulder from lifting up). Bend your neck to the right side as shown, and using your right hand, gently assist the stretch to the right.
You should feel a stretch down the left side of your neck. Repeat to the other side, holding each stretch for 30 seconds.
NB-If you feel pain on the right hand side whilst bending to the right, then please STOP, and consult your physio.
 6) Corner chest stretch-this stretch can’t be done in sitting, however it is one of the most important stretches to do as it stretches your chest, the culprit for your rounded shoulders.
6) Corner chest stretch-this stretch can’t be done in sitting, however it is one of the most important stretches to do as it stretches your chest, the culprit for your rounded shoulders.
As shown, stand facing a corner and place your elbows at about 90 degrees, forearms resting against the wall. Then step forward with one leg and allow your chest to fall in, towards the corner. You should feel a stretch in the front of your shoulder and into your chest. Hold 30 seconds and repeat 2-3 times.
 7) Lying McKenzi stretch- The last stretch I want you to do is one we often use in Physio to help people with lower back pain caused by a disc problem.
7) Lying McKenzi stretch- The last stretch I want you to do is one we often use in Physio to help people with lower back pain caused by a disc problem.
You should start by lying on your stomach with your arms at your sides. Gently push up onto your elbows at first, and allow your lower back to completely relax. Repeat 8-10 times.
As the stretch improves, you might be able to lock your elbows out as shown in the picture, but do this slowly as sudden extension may cause some pain.
This stretch also targets your hip flexors (front hip muscles) which get shortened over time by sitting.
NB-If you have pain referring down your leg/s or into your bum then please stop and see your physio
So there you have it, a few stretches to get you going and hopefully reverse some of your poor posture. You should try aim to do these stretches at least once a day (even if its not all of them at once) and the more often you do them, the less painful and more flexible you will become.
Ric @PhysioPRO
BY: Riccardo Vaccaro
Back injuries / Lower Limb injuries / Neck injuries
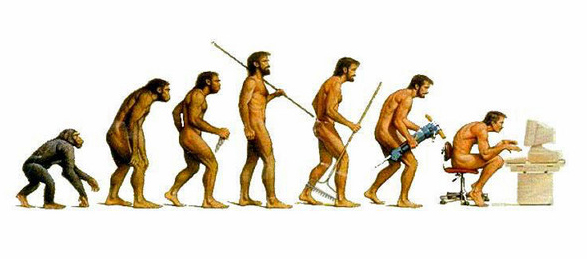
Sitting posture and the (D)evolution of man
FACT: Human beings were not designed to sit for hours on end…
Sitting posture is a constant topic that raises its “crooked” head up at nearly every physio appointment. Why? Well because as physiotherapists, we are constantly battling the negative effects of sitting for hours on end.

The human spine is divided into 4 distinct curves: neck (cervical), middle (thoracic), lower back (lumbar) and sacrum. These curves are designed to distribute the load that gravity places on the spine (like a spring), absorb shock and obviously allow movement.

The problem with sitting is that these curves are “imbalanced”. The neck and middle back curves become exaggerated and the lower back’s curve is almost completely lost (see pic above). This results in adaptive muscle shortening or stretching, depending on which side of the curve we look at. This then translates to poor standing posture and difficulty with functional movements, with the end result being an injury. So what im trying to say is the way you sit at your desk could very well be the reason why you pulled your hamstrings whilst you were running….

Another scary fact is the amount of pressure that you place on the discs (the “cushions” between the vertebras). As you can tell from the diagram above, the difference in pressure between standing and forward lean sitting (i.e. sitting on the edge of your chair leaning forwards) is an ASTONISHING 90% increase!!!! That’s the equivalent of having someone with your own body weight standing on your head!!!
So what can you do if you are one of those office bound monkeys? Well, start off by assessing your posture by comparing it to the “ideal” posture below. Make changes where you can and stick to those. You can have the most expensive “ergonomically” designed office chair, but if you’re not sitting in it properly it’s worthless.

Secondly, STAND!!! Every 30-40minutes, get up and walk around, or if you have some privacy try stretching a bit. Try standing whilst you talk on the phone or walk over to that colleague to deliver a message rather than sending an email.
Look out for my next article on some of the stretches you should be doing at the office or home to improve your posture.
Regards
Ric@PhysioPRO
BY: Riccardo Vaccaro
Back injuries / General Health/Fitness / Neck injuries
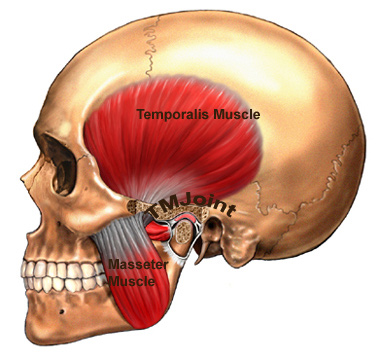
The TMJ- the little joint with a large role
The Temporomandibular joint (TMJ) is a little joint with a big name and even larger role to play in day to day life. It’s found between the jaw bone and one of the bones in the skull – just below the temples.

When one considers how much we use this joint in daily activities it isn’t very surprising that this joint is subject to wear and tear. This, because it’s involved in chewing and talking (ceaseless activities for some). The TMJ can even be damaged while a person sleeps, as clenching or grinding one’s teeth will cause the joint’s cartilage lining to wear away.
Common causes of TMJ dysfunction are:
- Poor posture i.e. one that sees the chin poke out
- Habitual or excessive chewing of gum
- Previous trauma to the area
- Dental problems
- Stress and clenching of teeth
TMJ dysfunction could see people experience limited motion and a general dull ache over the side of the face as well as local muscle tenderness. A ‘click’ may also be present as patients open and close their mouth, as the joint dislocates and relocates back into place. Headaches, sinus and neck problems can all be associated with TMJ dysfunction. It’s clearly a very important joint to keep clear of damage.
A quick self test for TMJ health:
- Place 3 fingers vertically into your mouth. Inability to do this indicates TMJ hypomobility.
Using physiotherapy to treat damage to the TMJ involves:
- myofascial release
- massage
- gentle stretches
- accessory mobilizations
- electrotherapy
- postural correction
- re-education.
Most important is identifying and addressing the cause of the dysfunction.
So if you think you are having problems in this particular area, do not fear. Help is always at hand. Visit your PhysioPRO practice for an assessment.
Until next time…Keep Smiling 🙂 and chewing and talking.
Andrew Savvides
PhysioPRO
BY:
General Health/Fitness / Neck injuries

The head work behind YOUR headache!
Most people have at some time or another suffered from headaches or know of someone close to them that have. For a lot of us though it’s not a regular thing, maybe we partied a bit too hard the night before or are just having a really stressful day, and we take some pain killers and carry on with our day to day lives. But for some it is a devastating condition that impacts on every part of their life, as well as the lives of those close to them. How many of you husbands out there have come home after a long days work and all you want to do is get “close and comfortable” with your wife, only to hear….not tonight honey…. I have a headache! Classic example.
The effects of headaches go a lot deeper than just the pain in the head. People suffer from a large amount of psychosocial factors, such as functional disability and loss of concentration, making work and studies a nightmare. They have a decreased productivity and emotional handicap which has a negative impact on close relationships and can lead to anxiety, anger and eventually depression. I mean when you are in pain you become miserable, and nobody wants to be around miserable people or even worse…..be that miserable person.
But there is hope, through a multi-disciplinary approach a lot of headache sufferers can be helped to lead normal, productive, happy lives.
Ok let’s talk a little bit about headaches. Firstly you get Primary headaches, which are not associated with other diseases and are the most common kind and then you get Secondary headaches, which are a symptom of an underlying ominous disease. Obviously these types of headaches are a lot more serious and here is the “Red Flag” list of things to look out for:
RED FLAGS
- Sudden onset of a new severe headache
- Progressively worsening headache
- Onset after exertion, straining, coughing or sexual activity
- Onset of first headache after 50 yrs old
If you have any of these symptoms please go and see your doctor immediately as your headache could be a warning sign of something a lot more serious!
PRIMARY HEADACHES
Why do we get headaches? How does it all work?
Well there are a lot of different triggers, both internally as well as externally that can lead to a headache. i.e. Muscular, Vascular , Temporomandibular joint (TMJ) or cervical dysfunction, stress, posture, certain foods, dehydration, sinuses, bright light, alcohol, hormonal changes, sleep disturbances and the list goes on.
These triggers are not necessarily what are causing the pain they just set it off, like a landmine. I was at a headache lecture the other night and the doctor explained it like this.
In your brain you have the trigeminocervical nucleus ,and what that big fancy name does is that it’s the principle centre of the head and neck involved in the transmission of nociceptive information .i.e “the headache generator”
So basically what all these different triggers do is sensitize the “headache generator” more and more until eventually it explodes like a landmine and sets of a headache. They have also found that in chronic headache sufferers the “headache generator” part of the brain is more sensitive to the incoming messages from the different triggers than non sufferers. So what we need to do to prevent these headaches from developing is to try and desensitize the “headache generator” by cutting down the amount of stimuli it is receiving from the triggers. But in order to do that you firstly have to identify your own individual triggers.
A good way of doing this yourself (and I highly recommend this), is to keep a headache diary, in order to discover your own individual headache pattern.
| Date | Time | Duration | Rate Intensity (1 to 10) | Possible triggers | What relieved headache? | Ability to function |
This will help you start picking up trends and understanding your headache better.
Two of the major internal triggers are firstly Muscular .i.e. trigger points (a hyperirritable spot in a taut band of muscle) mainly in the head and neck muscle groups, causing the Tension type headaches. Secondly the Vascular system, where the arteries in the scalp and skull vasodilate causing Migraines. Some migraine suffers experience either a visual disturbance, vertigo, numbness, weakness etc, prior to the onset of a headache. We call this an aura, which is caused by the blood vessels in the brain vaso-constricting. It is still unclear why this happens prior to the onset of these migraines.
Stress, Ergonomics and Posture are very big external triggers that need to be looked at and corrected.
Physiotherapy plays a major role in treating both the internal as well as external triggers along with a multi-disciplinary team of course. Helping to correct the muscular system and looking at correct ergonomics and posture as well as core stabilising exercises and manipulation therapy have been proven to give lasting relief to headache sufferers.
A lot of people turn to the medicine cabinet when a headache is knocking on the door to try and mask the pain. The medications used are either Preventative or Rescue medication. Rescue medication you take once you already have the headache e.g Simple analgesics (Asprin, Paracetomol), Triptans (Imigran, Maxalt) etc
Preventative medication on the other hand you take before the headache starts and is only prescribed for severe, regular headaches when nothing else is helping. Some examples are Trepiline(Anti-depressant), Epilum, Atenolol(beta-blocker) .
The problem with all these drugs is that some people don’t respond to them and many of them have really bad side effects. If patients get depend on the medication and are using them regularly they can also develop Medication Overuse Headaches which a lot of the times are worse than their original headache that they started with.
Myself being a physiotherapist, I believe that medication has a role in headache treatment but there are many other ways than just “popping a pill’(which just masks the pain and doesn’t deal with the true cause of the problem) to cure your headaches.
For instance I was at another course where the lecturer explained just by advising his patients to drink more water [(30ml/kg body weight /day) so if you weigh 60kg you should drink 1.8L of pure water a day] and keeping their blood glucose levels constant (by eating more low GI foods and smaller, regular meals during the day), almost all of their headaches had improved. Something small to think about…
Thank you for taking the time to read through this article. I hope it has benefited you in better understanding your headache and how to treat it.
Andrew@PhysioPRO
BY:
General Health/Fitness / Neck injuries

Reckless drivers can be such a Pain in the…Neck
The notorious Highveld showers having come with a vengeance this past rainy season, have wreaked havoc in many ways and forms… one form that I’d like to mention is the ‘Whiplash’ injury. Can one sustain this type of injury from rainfall…? Not directly, but some of us are noted for driving dangerously on wet roads (but we won’t point fingers here), and this often results in Motor Vehicle Accidents (MVA’s).
Whiplash is commonly associated with MVA’s, usually when the vehicle has been hit from the rear, however, the injury can be sustained in many other ways, including falls from height, rugby tackles etc.
‘Whiplash’ is a non-medical term describing a range of injuries to the neck caused by or related to a sudden distortion of the neck associated with extension.
Whiplash injuries are associated with varying degrees of pain to the neck and back, referred pain to the shoulders, sensory (Spinal cord) disturbances (such as pins and needles or heaviness) to the arms & legs and headaches. Symptoms can appear directly after the injury, but often are not felt until days (or even years) afterwards. Whiplash injuries are commonly graded from 1 – 5 depending of the presentation of the associated symptoms.
Treatment following a whiplash injury includes:
Seeing a physiotherapist or doctor as soon as possible (within 24hours) after injury. They will assess the extent of your injury by conducting: an injury history, a head and neck examination, and referral for X-rays to rule out any neck bone fractures.
A doctor will prescribe medication for pain, anti-inflammatories, muscle relaxants (maximum use of 3 weeks) and a neck soft collar (never longer than 72 hours as it may lead to prolonged inactivity).
Physiotherapy may in the acute stage include ice/heat/electro therapies to relieve pain and muscle tension. Soft tissue and joint mobilisations with appropriate exercises (for range of motion and strength), will also be used later as indicated. Encouragement to return to normal activities of daily living as soon as possible to maximize and expedite full recovery is our main aim after resolution of symptoms.
The consequences of whiplash range from mild pain for a few days (which is the case for most people), to severe disability caused by restricted head movements of the cervical spine, sometimes with persistent pain. Therefore, to ensure long term recovery and that the neck, upper back and shoulders do not become chronically painful, stiff and possibly debilitating, it is necessary to receive a course of quality physiotherapy care and be diligent in adhering to the rehabilitation and exercise program prescribed.
BY:
Neck injuries

“Chest out, Stomach In”…
Recently, I’ve become very conscious of the fact that I need to address the issue of my personal health and wellbeing (Read: “I really have to shed some kilo’s because I feel like an inert morsel, experiencing unexplained discomfort at times” ). Tired of uncomfortable, boring and outdated workout routines and aiming to get new information in order to enjoy working out again, I came across a thought provoking article online…”
Correcting Posture: Myth or Reality? by Anoop Balachandran (originally published at MindandMuscle.net ). Also see: http://www.exercisebiology.com.
Physiotherapists perform a postural assessment as part of their initial assessments. Deviations from an ideal posture, such as an exaggerated anterior pelvic tilt – will definitely lead to low back pain. A forward head or grossly rounded upper back posture will end in shoulder, neck, and upper arm pain. We have all heard of examples where posture is definitely linked to pain.
The belief of posture related pain conditions is quite widespread. Surprisingly though, there is little scientific evidence to show that ‘bad’ posture will cause pain. We see people with ‘bad’ postures with no pain, and many more with ideal posture in a lot of pain, this shows that there is much more to pain than just posture.
Classifying postures and making people believe that certain postures and movements are bad and dangerous, instills fear of these postures, and enhances pain by fear-avoidance patterns. In short, casual conclusions about pain and posture could be doing more harm than good.
As Physiotherapists we are trained to look for common postural problems and then correct these where necessary. We are also focused on attempting to show a person struggling with pain that they are not doomed to a painful future because of their less than ideal posture but rather an aversion to mobility and normal function. So, the key to long-term alleviation of related pain is management by ‘physical therapy’ not just a passive reception of treatment.
In essence we must note that…
– There is no ‘perfect’ posture.
– Pain isn’t always caused by muscle imbalances (tightness or weakness).
– Pain is much more complicated than just stretching and strengthening the right muscles.
– The body doesn’t do well with prolonged periods of immobility.
– To break the immobility-pain cycle – we encourage movement and never restrain it.
– Corrective postural therapy (such as the various physiotherapy pain – relief modalities and ergonomics) can be effective but must always include movement and functional activities (commonly referred to as exercises).
Yours in Health
Mitesh
BY:
Back injuries / General Health/Fitness / Neck injuries