

Prevention is better than Cure
I’m sure many of you out there have heard of the acronym “RICE” which is used by athletes all over the world post acute injury. Where the R = Rest, I = Ice, C = Compression and the E = Elevation. One other very important letter can be added to this acronym which can have a huge impact on the athletes sporting career and well being…that letter is P…changing the acronym to “PRICE” with the P representing Prevention.
If we can prevent or at least minimise an athlete’s potential for injury our work as sports physiotherapists is half done.
The International Federation of Associated Football (FIFA) recognized this and developed an injury prevention warm up program known as “FIFA 11+” mainly to prevent ACL (Anterior Cruciate Ligament) tears. The program is divided into 3 Sections:
- Part 1: focusing on slow speed running exercises with active stretching and player contact.
- Part 2: Six sets of exercises each with 3 levels of difficulty focusing on core and leg strength, balance and plyometrics.
- Part 3: Moderate to high speed running exercises combined with planting/cutting movements.
To download the full program please visit the FIFA 11+ site http://f-marc.com/11plus/home/
Things to remember: you need to be 14 yrs and older to start using the FIFA 11+ program and always use proper technique during all of the exercises, focusing on your form and posture.
For a prevention program to be beneficial it needs to be done at least twice a week and the exercises should be sport specific focusing on plyometrics, balance and strengthening.
So till next time remember…Prevention is better than Cure!
Andrew@PhysioPRO
BY:
Knee injuries
ITBFS – Iliotibial Band Friction Syndrome
Lateral knee pain (pain felt on the outside of the knee) is a common problem especially among long distance runners and cyclists.
The most common cause of lateral knee pain is probably iliotibial band friction syndrome (ITBFS). Other causes include lateral meniscus abnormalities, patellofemoral syndrome, biceps femoris tendinopathy (one of the hamstring muscles) and superior tibiofibular sprain. In some cases the pain could even be referring from the lumbar spine.
With so many possible causes of lateral knee pain, it is vital to make the correct diagnosis by
a) looking at the mechanism of injury – in other words how you hurt yourself
b) looking at the activity that brings on the pain
c) having specific tests done by your physiotherapist
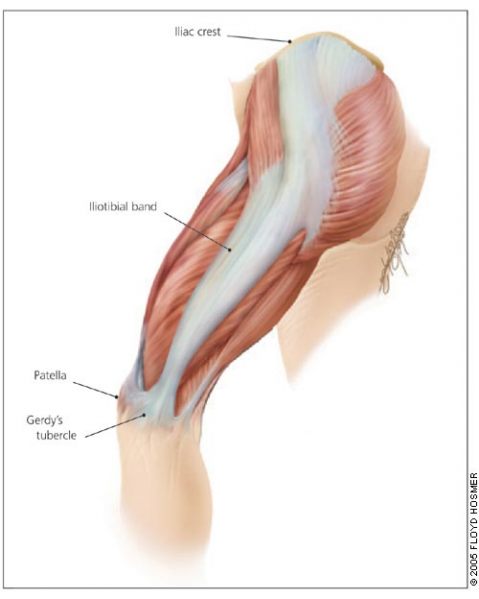
Your Iliotibial band (ITB) is a lateral thickening of the fascia surrounding your thigh. Proximally at the hip the tensor fascia lata muscle inserts into the ITB, as does a portion of the gluteus maximus muscle. Distally the ITB inserts onto the patella and tibia. Thus you can see by its attachments that it plays a role in lateral stability both at the knee and the hip joints.
The ITB has many functions
- Stabilising the pelvis in stance
- Flexion (bending), abducting (moving to the side away from the body) and medial rotation (turning inwards) of the hip
- Stabilising the knee in extension (when its straight)
- Lateral rotation (turning outwards) of the tibia on the femur

Iliotibial band friction syndrome (ITBFS) is an overuse injury presenting as lateral knee pain that is exacerbated by sporting activity. Tenderness is elicited over the lateral femoral epicondyle which is 2-3 cm above the lateral joint line of the knee. The pain often develops at the same time or distance during the aggravating activity. A change in training methods or shoes, longer training and downhill running are often aggravating factors.
Obers test (which would be done by your physiotherapist) would reveal ITB tightness and quite possibly the patient would have tightness and shortening of the tensor fascia lata and gluteus maximus musles, which as discussed earlier, are attached to the ITB.
Treatment with ice and electrotherapy or corticosteroid injection should not only be focused locally on the lateral knee but foot and hip biomechanics should be looked at for more favourable long term results. It has been shown that runners with ITBFS can have significantly weak hip abductors in the affected limb, so focusing on correcting the underlying weakness and fatigability in these muscles is quite important. Myofascial release of the ITB, tensor fascia lata and gluteal muscles as well stretching these muscles is very beneficial. Dry needling and use of a foam roller may also be recommended.
The last resort – if all conservative management fails – is surgery. But before you decided to go under the knife visit your physiotherapist and see if they can’t provide a solution that works for you.
Andrew@PhysioPRO
BY:
Knee injuries / Lower Limb injuries

Patellar Dislocation
This unfortunate injury is associated with sports that involve repetitive running, jumping, or kicking such as soccer and rugby.
 The patella (kneecap) is a loose bone that sits in your quadriceps and patella tendons. It glides up and down a groove (the trochlea groove of the femoral condyle) as you bend and straighten your knee.
The patella (kneecap) is a loose bone that sits in your quadriceps and patella tendons. It glides up and down a groove (the trochlea groove of the femoral condyle) as you bend and straighten your knee.
Patellar dislocation occurs when the patella is displaced from this groove, most commonly laterally (towards the outside of the knee). This may either be caused by something traumatic especially where there is a history of a traumatic force to the kneecap or it can occur in the absence of trauma as is the case in young girls with associated ligamentous laxity
The stabiliser in your kneecap that protects against displacement is the medial patellofemoral ligament. Anatomically it acts as a passive check to prevent the patella from extreme lateral displacement which is why we find that in the majority of dislocation cases it is disrupted.
Patients usually complain of the knee suddenly giving way while jumping or running/twisting and the subsequent development of severe pain. A feeling of something “moving out of place” or “popping” is quite common. Often the dislocation reduces spontaneously with knee extension. But, swelling develops almost immediately.
It is common to mistake this injury for an Anterior Cruciate Ligament ( ACL) rupture as both conditions have similar mechanisms of injury with an audible “pop” and giving way of the leg as well as a quick development of swelling. But, on examination of a patellar dislocation there is usually gross swelling, marked tenderness over the medial (inside) border of the patella and when attempting to push the patella in a lateral direction the patient experiences pain or apprehension. Quadriceps muscle contraction aggravates the pain.
Most first-time dislocations are treated without surgery, with pain relief medication, immobilization of your knee with an extension splint for 2-3 weeks. During this time period you should be using crutches, and be following a rehabilitation program.
The most important aim of rehabilitation after such an injury is to reduce the chances of a recurrence. Hence the rehab program is lengthy and emphasizes core stability, vastus medialis obliquus strength, and stretching of the lateral structures when tight.
Surgery is indicated for second dislocations, or in patients not improving with appropriate rehabilitation (the re-dislocation rate after primary patellar dislocation managed non-operatively is anywhere between 15-44%). Medial patellofemoral surgery has become the surgery of choice.
So if you find yourself “buckled at the knees”, follow the RICE principle in the acute stage (Rest, Ice, Compression and Elevation) and seek treatment from your physiotherapist and/or orthopaedic doctor.
Andrew@PhysioPRO
BY:
General Health/Fitness / Knee injuries / Lower Limb injuries

Achilles Tendinopathy
The Achilles tendon is made up of the combined tendons of the gastrocnemius and soleus muscles (the two calf muscles). It is the thickest and strongest tendon in the body. But, that doesn’t make it immune to injury. Even the legendary Achilles – amongst the strongest and bravest Greek warriors – met his untimely demise following an injury to his Achilles tendon.
Injury to the Achilles tendon occurs when the load applied to the tendon exceeds the ability of the tendon to withstand that load. It is most common among males aged 30-50. These over-use Achilles tendon injuries may arise with increased training volume or intensity, change in training surface or footwear or decrease in recovery time between training session.
An athlete’s biomechanics might also predispose them to Achilles tendinopathies. These biomechanics include excessive pronation or supination of the foot (where the foot tends to fall inwards towards the arch or be pushed outwards), calf weakness and altered tibial or femoral mechanics etc.
Most of the time the athlete will notice a gradual development of symptoms, complaining of morning stiffness and pain, which diminishes with walking and application of heat. The two common sites of pain are the midportion of the Achilles tendon and the insertion of the Achilles tendon at the calcaneus.
One of the first things to look at when treating these problems is to identify and correct any predisposing factors i.e. training methods, footwear, orthotic and biomechanical correction.
Once these have been addressed the athlete should commence an eccentric training program, where they focus on controlling the negative motion of the repetition i.e. where the muscle is working in a lengthened state. The Alfredson painful heel-drop protocol for Achilles tendinopathy has shown to be very successful in treating midtendon Achilles pain. It consists of two main exercises – the ‘gastrocnemuis drop’(knee fully extended) and the “soleus drop”(knee bent to 45 degrees). Both exercises start on a step with the calf in a raised position. From this position the patient slowly lowers the heel so that the foot is parallel to the ground. Patients should do 3 sets of 15 repetitions twice daily for 12 weeks everyday of the week.

Patients should not be put off by the fact that the pain may worsen at the start of the program as this is part of the normal recovery process. If a patient experiences no pain during the exercises, they are advised to increase the load until the exercises provoke some pain i.e. add a weighted backpack. If you are suffering from pain at the insertion of the Achilles tendon then you should do a similar exercise program but remove the step, just do it standing on the floor, as this has been shown to be more effective.
With the correct treatment approach and the guidance of your physiotherapist, Achilles tendinopathy can be successfully managed and overcome.
Andrew@PhysioPRO
BY:
Ankle injuries / Foot injuries / Lower Limb injuries

A MUST-DO stretch
Now before you start panicking, NO, we are not going to be doing the stretch you see above, but we are going to show you a REALLY important stretch…
Most people are aware of the importance of stretching, and we have covered the topic on the benefits of stretching in an older post that you can read here, but what I would like to focus on today is the importance of stretching your HIP FLEXORS. As a Physiotherapist, I consider this muscle group to possibly be the most important muscle group to stretch, as it not only affects athletic ability but also your posture, and subsequently, chronic pain.


First for some anatomy. Your hip flexors are comprised of 3 distinct muscles namely: Iliacus, Psoas Major and Rectus Femoris (bet you probably never heard of them?).
Iliacus and Psoas Major (often grouped together and called Iliopsoas) are pure hip flexors (bringing your knee to your chest), whilst Rectus Femoris is a hip flexor and knee extensor (as it crosses both the hip and knee joint).
If you have a look at the first picture above (left), you will notice that the Psoas muscle is attached to the lower part of your spine. Thus, if it is tight, it actually pulls your spine down and exaggerates the curve of your lower back (anterior pelvic tilt). Together with the other two muscles being tight, this can account for “hyperlordosis” and lead to lower back problems and pain.

So why do they get so tight? Surely if you are not exercising these muscle, there is no reason for them to become overly tight?
There are two main causes for this. Firstly, we sit way too much, and secondly, we all like to have a six-pack, so if we do get a few minutes to exercise, we tend to do sit ups…
Now I’ve said it before, “Humans were just not designed to sit all day long!”, so for the majority of people that sit most of their day, these hip flexor muscles are in their shortened position for hours on end, and as a result, they become shortened and tight. Then when you do finally stand up, they are “fixed” in this position.
The second point was on sit ups and most other stomach exercises. Most people don’t realize this, but if you do a standard sit up (i.e. lying on your back, knees bent and then curling your back to bring your chest to your knees), your hip flexors are doing about 70% of the work…. Whether you bring your chest to your knees, or your knees to your chest, its the same movement– HIP FLEXION! (on a side note, thats the reason a lot of people get lower back pain when doing sit ups-tight hip flexors).
So here come the Rescue Remedy:
Its called many different names, but we like to call it the PROPOSAL STRETCH- for obvious reasons

I teach 2 different ways of doing this, either as you see above (more effective as you are bending the knee as well, so you are also stretching Rectus Femoris), or by placing your back leg on a chair (below). If you are doing it right, you should feel the stretch in the front of your hip, and possibly also slightly on the front of your thigh. People that do a lot of squatting movements (Crossfit, gym, skiing etc), or lunges (squash, tennis etc) would benefit immensely from this stretch, as It could limit your ability to get into those positions.

Hold this for 30 seconds and repeat for 3 sets, at least 2-3 times a day (more if you are sitting all day long).
Happy Stretching
Ric@PhysioPRO
BY: Riccardo Vaccaro
Back injuries / Hip injuries / Lower Limb injuries

Acute Hamstring Strains
The hamstring muscle is in fact a group of three muscles – the semimembranosus and semitendinosus medially (more inward) and the biceps femoris laterally (more outward) which is divided into a long and short head. ( see picture)

A substantial force is usually required to develop an acute muscle strain in the hamstrings. This is so much the case that individuals can typically recall precisely when their injury took place. A few risk factors are listed below:
- Age – the older athlete has an increased risk of acute hamstring strains.
- Previous injury – a prior history of acute hamstring strain increases the risk of future injury
- Hamstring:Quadriceps strength ratio – the weakness or strength of the hamstrings and quadriceps n relation to each other are seen as a risk factor.
- Poor lower limb proprioception( knowing where your limb is in space)
There are 2 distinctly different types of acute hamstring strains. The more common of the two, Type 1 hamstring strains usually occur during high speed running when the hamstrings is working eccentrically and involve the long head of biceps femoris most commonly at the upper muscle-tendon junction. These types of strains seem worse in the early stages of the injury with a marked acute decline in function but respond well to treatment and typically require a shorter rehabilitation period than the type 2 hamstring strains.
Type 2 hamstring strains occur during movements leading to extensive lengthening of the hamstrings into hip flexion such as high kicking or sagittal ( front) splits and are typically located close to the ischial tuberosity (high up the leg, in the bum region) and involve the uppermost free tendon of semimembranosus. These types of injuries can have less dramatic acute limitation but their rehabilitation period is often longer than that of type I strains.
The most common cause of posterior thigh pain is hamstring muscle strains but that does not rule out referred pain into this area from other structures such as the lumbar spine, the sacroiliac joint and trigger points in the gluteus minimus and meduis, as well as the piriformis muscles.
Management of the acute hamstring strain starts off in the acute phase by following the RICE (rest, ice, compression, elevation) principles in the first 48 hours as well as commencing with early pain-free muscle contractions. Subsequently recovery moves onto moving onto stretching, neural mobilisation, soft tissue treatments, strengthening and assigning a running program and/or individualised sport-specific training.
Acute hamstring strains are common injuries in most popular sports and have a very high recurrence rate of injury. Therefore having a good prevention program is essential. It has been suggested that a balance/proprioception program, regular soft tissue therapy and eccentric hamstring exercises may help prevent hamstring injuries.
Some of the best eccentric exercises for prevention of hamstring strains are Nordic Drops and Askling’s gliding exercises and it’s important to see your physiotherapist for assistance in this regard. But, be aware that in those new to eccentric muscle training, it can result in muscle damage and delayed onset muscle soreness. Therefore, any eccentric strengthening program should factor in adequate time for recovery.
Andrew@PhysioPRO
BY:
Hip injuries / Knee injuries / Lower Limb injuries

Aerobic vs Anaerobic Training
Training is the pursuit of any activity that will ultimately lead to an increase in performance in a specific sport. That’s what we mean when we talk about training!
So, training should be directed at bettering performance in an athlete’s chosen sport. As physiotherapists we should identify the most important components of fitness for each particular sport and tailor an athletes training toward improving these particular components.
Different training methods exist. These include aerobic training, anaerobic training, plyometric training, agility training, strength and power training – the list goes on. Today we are going to talk specifically about two of the most common types of training…. aerobic and anaerobic training.
Aerobic training or endurance training is performed to increase aerobic capacity or fitness. We measure aerobic capacity by measuring VO2 Max or the maximum oxygen an individual is able to utilize in one minute, per kilogram of body weight. VO2 Max can be measured in a fancy laboratory, but unfortunately most of us don’t train in this sort of setting, rather opting for the sports field or the gym. Luckily there is a simpler, albeit less exact method, known as predicted VO2 max which is estimated by measuring the heart rate at a specific workload which is a method commonly used.
It’s reported that aerobic training effects occur while maintaining a heart rate of between 70% and 85% of one’s maximum heart rate. Maximum heart rate is estimated by subtracting your age from 220. So it is pretty easy to do: for a 30 year old like me, max heart rate would be 220-30=190 beats per minute. And the ideal range of heart rate for me to produce an aerobic effect would be between 135 (70%) and 160 (85%) beats per minute.
And you thought jocks didn’t do maths!
Many sportspeople find benefit in the endurance and fitness gains made by training aerobically as well as the health benefits of a stronger cardiovascular system and resultant weight loss.
Anaerobic training burns glucose as an energy source but does this without oxygen present, to produce energy. Oxygen is absent because this sort of training is typically high intensity for a short period of time and there isn’t time for full oxygen delivery to the muscle cells using the glucose. This pathway utilizes ATP as its energy substrate. The process produces less energy per molecule of glucose utilized than aerobic exercise does when burning up that glucose with oxygen present.
Anaerobic training improves the capacity to maintain a high rate of power production at very high intensities for short period of time. This type of training helps maintain muscle recruitment and muscle contractile function after training so that the onset of fatigue is delayed, as well as improving the body’s tolerance to lactic acid build up. Lactic acid is a by-product of training anaerobically and contributes to the discomfort felt while training.
Interval training or intermittent exercise is the most efficient method of increasing anaerobic fitness. Such training involves bouts of exercise separated by periods of rest or recovery. The principle behind this type of training is to achieve a level of lactic acidosis with one individual effort and then allow the body to recover from its effects before embarking on another bout of exercise. This is done to train the body to cope with higher levels of lactic acid before shutting down and to recover faster.
As mentioned, to obtain maximum gains from interval training it must be activity/sport specific. Also remember that because of its increased intensity, the potential for injury is a little higher than that presented by aerobic training. It’s therefore beneficial for athletes to use a variety of training methods to take advantage of the benefits offered by each and allow time for rest and recovery of the body.
Andrew@PhysioPRO
BY:
General Health/Fitness / Lower Limb injuries / Upper Limb injuries

Hypermobility- a quick test to see which side of the spectrum you’re on
Our bodies are all different. Some are tall, some short, some big, some small and the same variety is found when it comes to the tissues within. Some people have more collagen in their ligaments and tendons which means they tend towards being more rigid and stiff. Others have less collagen and are far more flexible. As with most things in life, problems can occur on either extreme.
Let’s deal with one side of the spectrum – being very flexible or ‘hypermobile’. The problem here is that increased laxity or flexibility in the joints makes the joints more unstable and puts a person at a greater risk of injury, especially for those involved in contact sports. As we get older the body naturally stiffens up so hypermobile individuals that avoid injury early on in life are generally able to be more active older adults.
The Nine-Point Beighton Hypermobility Score is a quick and easy test to rate how hypermobile you are. It’s a simple 9 point system where the higher the score the higher the laxity. It is scored as follows:

Scoring high on the Beighton scale doesn’t necessarily mean you have Hypermobility syndrome as you could be hypermobile with no adverse symptoms (which include pain in the muscles and/or joints). Generally if you score either 4 or 5 out of 9 you are on the hypermobile end of the spectrum and should take precautions to prevent injury and work on stabilising and proprioceptive exercises, such as balancing on different surfaces while performing sports specific exercises, so that you can stay fit and healthy into your old age.
BY:
General Health/Fitness / Lower Limb injuries / Upper Limb injuries

Recovery Rules
With the Olympics currently in full swing, I’m sure many of you are enjoying all the top class sport showing on our televisions. Olympic athletes compete at the highest levels for consecutive days – sometimes even twice in the same day. How quickly and how well they RECOVER is vital for their optimal performance and could be the difference between going for Olympic gold and going home early.
The main aim of a post-game/event program is to enhance recovery, to maximize performance and minimize potential for injury at the next event. Recovery programmes have the following objectives:
- Restoration of function
- Neuromuscular recovery
- Tissue repair
- Resolution of muscle soreness
- Psychological recovery
A number of recovery methods are used by sportsmen and woman. Though there’s limited research in to the efficacy of most of them, let’s look at a few of the most popular techniques used:
Warm-down (active recovery)
Most athletes perform a warm-down of between 5 and 15 minutes after intense exercise followed by stretching of the muscles used in their specific sport. The warm down is also generally specific to the nature of their particular sport.
Cold Water Immersion (CWI)
 As the name suggests, players immerse themselves in ice baths ranging from 5-15°C for up to 5 minutes at a time. This has a cooling effect on the body tissues. CWI is associated with a peripheral vasoconstrictive response, reduced perfusion, and a decrease in oedema (which all help control the inflammatory response). However sportsmen with a history of cardiac problems such as arrhythmias should avoid CWI as it results in “cold shock” with associated increase in heart rate, blood pressure, respiratory minute volume, and metabolism, thus placing extra stress on the cardiac system.
As the name suggests, players immerse themselves in ice baths ranging from 5-15°C for up to 5 minutes at a time. This has a cooling effect on the body tissues. CWI is associated with a peripheral vasoconstrictive response, reduced perfusion, and a decrease in oedema (which all help control the inflammatory response). However sportsmen with a history of cardiac problems such as arrhythmias should avoid CWI as it results in “cold shock” with associated increase in heart rate, blood pressure, respiratory minute volume, and metabolism, thus placing extra stress on the cardiac system.
Massage
Intense training causes prolonged elevation of muscle tone in both resting and contracted states. This increased tone or “muscle tightness” limits the extensibility and shock absorbency of soft tissue and thus predisposes the tissue to strain. Active trigger points that result from heavy training may reduce muscle strength. All these problems can impair training and competition and can progress to injury if they are not resolved. Soft tissue therapy is thought to work by reducing excessive post-exercise muscle tone, increasing muscle range of motion, increasing the circulation and nutrition to damaged tissue, and deactivating symptomatic trigger points. It also helps to identify any soft tissue abnormalities, which if untreated could progress to injury.
Nutrition
Nutrition aids in the recovery from intense exercise by replenishing glycogen stores and providing necessary protein and water. Repetitive bouts of activity can cause profound glycogen depletion and substantial breakdown of muscle proteins which could lead to impaired sporting performance. Athletes are encouraged to consume a carbohydrate rich snack/meal that provides 1-1.2g of carbohydrate per kg of body weight as well as 10-20g of high-quality protein within the first hour post exercise, as this is when rates of glycogen synthesis are greatest. Glycogen is the major energy source for muscular activity in the body. Large amounts of fluid may be lost during exertion, especially with increased intensity and in hot conditions. Rehydration is vitally important to replace the lost fluid as well as electrolytes (especially sodium) lost through sweat.
Deep-water running
This recovery method involves running in the deep end of a swimming pool using a buoyancy vest. It is a form of cross-training that reduces the impact put on your joints and thus reduces overuse injuries.

Compression Garments
Lower limb tights and below-knee socks are advised for athletes soon after finishing their event. Athletes should leave them on for the next 24 hours. This aids in recovery from post-event muscle soreness.
Lifestyle factors such as adequate rest and sleep as well as the psychology of the athlete have also shown to influence recovery times.
As you can see what the athlete does off the track/field might be as important as what they do on it and coaches should be encouraged to incorporate recovery time into athletes’ schedules.
Andrew@PhysioPRO
BY:
General Health/Fitness / Lower Limb injuries / Upper Limb injuries