

Increase your running distance safely
How to safely increase your running distance
With summer just around the corner, most people have started getting ready for their beach body. You may have taken up any number of sports to achieve this, but certainly, the most common “seasonal sport” is running. Running is a relatively cheap, easily accessible sport, but if you are not careful with how you increase your distance it could turn into a costly exercise…
Most runners have heard of the 10% rule. This states that you should never increase your distance by more than 10% from the previous week. This “rule” has not been validated by science and a recent article published in the Journal of Sports and Orthopaedic Physical Therapy, revealed some interesting findings.
The study followed 874 novice runners for 1 year and gave each runner a GPS watch to track their distance. Based on their weekly running increase, they were placed into one of three groups: less than 10%, 10%-30% and more than 30%. In total 202 participants sustained an injury over the course of 1 year and what will surprise most is that the total number of injuries per group were not much different.

Yes, there was an increase in the number of distance related injuries in the group that increased by more than 30% compared to the group that increased by less than 10%. So injuries like patellofemoral pain (runners knee), iliotibial band syndrome, medial tibial stress syndrome (shin splints), gluteus medius injury, greater trochanteric bursitis, injury to the tensor fascia latae, and patellar tendinopathy (jumpers knee) were more common in the group that increased training distance by more than 30%.
A possible explanation for this is that when you increase your distance, your running speed decreases (especially if you get fatigued). If your speed decreases, you have to take more steps to complete a given distance and the increased number of steps equates to increased “wear and tear”.
However, this was not true for all injuries. Injuries like plantar fasciitis, Achilles tendinopathy, calf injuries, hamstring injuries, tibial stress fractures, and hip flexor strains were just as common in all 3 groups. These injuries may be linked to running pace rather than distance, and its only through more research that these answers will be revealed.
So, all that science can presently advise is that you progress your weekly distances by less than 30% per week over a 2-week period.
Train smartly!
Ric@PhysioPRO
Article by Rasmus et al, titled “Excessive Progression in Weekly Running Distance and Risk of Running-Related Injuries: An Association Which Varies According to Type of Injury” J Orthop Sports Phys Ther 2014;44(10):739-747. Epub 25 August 2014. doi:10.2519/jospt.2014.5164
BY: Riccardo Vaccaro
Ankle injuries / Foot injuries / Hip injuries / Knee injuries / Lower Limb injuries

Exercising for Knee pain
In May 2012 I wrote an article on “The risk factors in knee pain”. In this article I discussed a study which showed the relevant risk factors in developing ANTERIOR knee pain, or otherwise known as Patello-Femoral Pain Syndrome (PFPS). You can read the article by clicking HERE.
In this study, one of the five risk factors that were found to be associated with PFPS, was “STRENGTH”, specifically that of the Quadriceps muscles which straighten your knee. Some of the advice then given was to strengthen your quadricep muscle through exercises such as squats and resisted knee extension.
Now, in a more recent study which examined the amount of strain placed on the Patello-femoral joint (knee-cap) during different exercises (squats and knee extension), researchers were able to conclude that there are “safe” ranges of motion during these exercises as well as “unsafe” ranges, which would either place a little or a lot of strain on the Patello-femoral joint.
: 
Results:
What the above image demonstrates is that during a squat movement, the “safe” range of motion is between 0 and 45 degrees of knee bending, and the “unsafe” zone from 45 to 90 degrees of bend. So when performing a squat to strengthen the quadricep muscle in PFPS, ONLY GO HALF WAY DOWN!
However, when performing a seated knee extension exercise, the “safe zone” is from 45 to 90 degrees, and the “unsafe zone”, 0 to 45 degrees of bend. So when performing a resisted leg extension exercise, ONLY GO HALF WAY UP!
By training in the “safe” zones for both of these types of exercises, you can strengthen your quadriceps muscles and at the same time, avoid feeling knee pain. If you are already experiencing pain under your knee cap, always consult your Physio prior to starting these exercises. Once you can do these exercises pain free, your Physio will progress them accordingly.
Ric@PhysioPRO
Article by Powers et al, titled “Patellofemoral Joint Stress During Weight-Bearing and Non–Weight-Bearing Quadriceps Exercises,” J Orthop Sports Phys Ther 2014;44(5):320-327. Epub 27 March 2014.doi:10.2519/jospt.2014.4936
BY: Riccardo Vaccaro
Knee injuries / Lower Limb injuries

Glorious Gluteus Muscles!
Back in 2011 I wrote an article called “How your BUM controls your BODY”. In the article I explained why the gluteus muscles are such an important muscle to train because it directly affected your ankles, knees and hips. If you haven’t already read it, then I suggest you go read it by clicking here.
In about 90% of lower leg injuries, I find that these gluteus muscle needs strengthening, so its crucial if you have any of those conditions mentioned in the previous article. In the article I only showed one exercise to do that targeted that gluteus muscle. Today I want to give you some more so you can really work it.
Advanced Clam


The starting position for this exercise is much the same as for the original Clam shell exercise (lying on your side,knees bent and heels touching). Place your forearm on the floor and then “push” your bottom knee into the floor, forcing your body to lift up off the floor-similar to a side plank. Now move the top knee up and down, but keep the heels touching.
The difference here is that you are training BOTH bum muscles at the same time. The bottom leg’s bum muscle is having to hold you up whilst keeping static (isometric) whilst the top leg’s bum muscle is moving the top leg (concentric). Trust me, it’s a real killer and you should feel the burn in your bum, right behind your hip. Once you can do 3 sets of 15 reps, then try adding an elastic band around your knees. An added advantage of this exercise is that is also trains your core at the same time!

This one looks easy but don’t be fooled… Stand with one leg over the edge of a step. Now keeping both knees LOCKED OUT STRAIGHT, lower your one leg by dropping your pelvis down on that side (keep those knees straight!). Now lift that leg as high up as you can and repeat. You want to concentrate on slowly lowering the leg (eccentric movement), and you should feel a burn in the gluteus muscle of the leg that you are standing on. Again, do 3sets of 10-15, but the slower you go the better.
So there you have it, two more exercises to add to your prevention program! And to all my CrossFit Athletes, this WILL help with your squat form! Tight buns
Ric@PhysioPRO
BY: Riccardo Vaccaro
Foot injuries / Hip injuries / Knee injuries / Lower Limb injuries

Osgood-Schlatter lesion
Anterior knee pain is a common complaint among sportsmen. One of the main causes of anterior knee pain in younger athletes is a condition known as Osgood-Schlatter lesion.
This condition is extremely common in teenage boys with a high level of physical activity, generally occurring at the time of a growth spurt. Mainly associated with sports involving a lot of running and jumping e.g. basketball, soccer, gymnastics etc.
 Examination reveals tenderness and pain over the tibial tuberosity (a small outgrowth on the shin bone where the patellar tendon attaches), with associated tightness of the quadriceps muscle. Excessive subtalar pronation (flat feet) may predispose the adolescent to the development of this condition.
Examination reveals tenderness and pain over the tibial tuberosity (a small outgrowth on the shin bone where the patellar tendon attaches), with associated tightness of the quadriceps muscle. Excessive subtalar pronation (flat feet) may predispose the adolescent to the development of this condition.
The pain is mostly aggravated by exercise and thus the management of the condition requires the athlete to modify their activity levels i.e. the less activity they do, the less pain they will have. Osgood-Schlatter lesion is a self-limiting condition, which means with time it will resolve by itself but may take up to 2 years. This can be very frustrating for the athlete and parents especially if they do not understand the nature of the condition. In the long term the athlete may develop a thickening and prominence of the tibial tubercle which will present as a bump on their shin bone just below the knee.
When the athlete is suffering from pain the symptomatic management includes icing the region, electrotherapy, massaging and releasing the quadriceps muscle, stretching as well as correcting any subtalar pronation if present.
So if you are suffering from this condition head to your local physiotherapist for advise and treatment.
Andrew@PhysioPRO
BY:
Knee injuries / Lower Limb injuries

Balance is the key
Ankle injury is arguably the most common sport injury. I tend to see a lot of patients coming into the practice complaining of repetitively “twisting “ their ankles. They will frustratingly announce ”that’s my bad ankle…I’m always twisting it” upset that they can’t seem to shake off the injury.
 Most of the time the reason for these continuous ankle problems, is a history of inadequate rehabilitation, especially in the aspect of balance and proprioception. Proprioception being the sense of knowing where a body part is in space, which is commonly lost after spraining an ankle. So if this is not properly re-taught, the patient is more likely to re-injure that same ankle when they return to sport.
Most of the time the reason for these continuous ankle problems, is a history of inadequate rehabilitation, especially in the aspect of balance and proprioception. Proprioception being the sense of knowing where a body part is in space, which is commonly lost after spraining an ankle. So if this is not properly re-taught, the patient is more likely to re-injure that same ankle when they return to sport.
In the initial returning to sport phase ankle braces and strapping can be used to add additional support as well as aid in proprioception of the ankle.
Exercises such as standing on one leg and trying to balance, progressing to closing your eyes while standing on the injured leg as well as standing on an unstable surface such as a balance board will all help improve your proprioception and balance.

Once you are comfortable with these more basic exercises you can now progress to more sport specific balance exercise. Focusing on keeping your balance while performing movements’ specific to your sport, the exercises are limitless.
The problem being most patients, once the pain is gone, stop there and don’t continue with the full rehabilitation program. So if you want to prevent those recurring nagging ankle injuries remember balance is the key.
Andrew@PhysioPRO
BY:
Ankle injuries / Foot injuries / General Health/Fitness / Lower Limb injuries
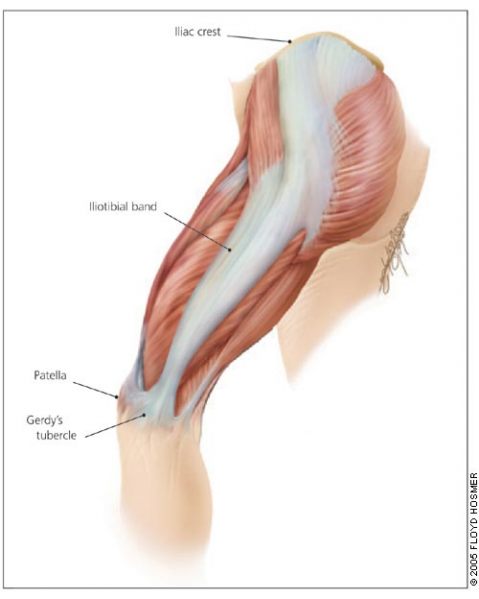
ITBFS – Iliotibial Band Friction Syndrome
Lateral knee pain (pain felt on the outside of the knee) is a common problem especially among long distance runners and cyclists.
The most common cause of lateral knee pain is probably iliotibial band friction syndrome (ITBFS). Other causes include lateral meniscus abnormalities, patellofemoral syndrome, biceps femoris tendinopathy (one of the hamstring muscles) and superior tibiofibular sprain. In some cases the pain could even be referring from the lumbar spine.
With so many possible causes of lateral knee pain, it is vital to make the correct diagnosis by
a) looking at the mechanism of injury – in other words how you hurt yourself
b) looking at the activity that brings on the pain
c) having specific tests done by your physiotherapist
Your Iliotibial band (ITB) is a lateral thickening of the fascia surrounding your thigh. Proximally at the hip the tensor fascia lata muscle inserts into the ITB, as does a portion of the gluteus maximus muscle. Distally the ITB inserts onto the patella and tibia. Thus you can see by its attachments that it plays a role in lateral stability both at the knee and the hip joints.
The ITB has many functions
- Stabilising the pelvis in stance
- Flexion (bending), abducting (moving to the side away from the body) and medial rotation (turning inwards) of the hip
- Stabilising the knee in extension (when its straight)
- Lateral rotation (turning outwards) of the tibia on the femur

Iliotibial band friction syndrome (ITBFS) is an overuse injury presenting as lateral knee pain that is exacerbated by sporting activity. Tenderness is elicited over the lateral femoral epicondyle which is 2-3 cm above the lateral joint line of the knee. The pain often develops at the same time or distance during the aggravating activity. A change in training methods or shoes, longer training and downhill running are often aggravating factors.
Obers test (which would be done by your physiotherapist) would reveal ITB tightness and quite possibly the patient would have tightness and shortening of the tensor fascia lata and gluteus maximus musles, which as discussed earlier, are attached to the ITB.
Treatment with ice and electrotherapy or corticosteroid injection should not only be focused locally on the lateral knee but foot and hip biomechanics should be looked at for more favourable long term results. It has been shown that runners with ITBFS can have significantly weak hip abductors in the affected limb, so focusing on correcting the underlying weakness and fatigability in these muscles is quite important. Myofascial release of the ITB, tensor fascia lata and gluteal muscles as well stretching these muscles is very beneficial. Dry needling and use of a foam roller may also be recommended.
The last resort – if all conservative management fails – is surgery. But before you decided to go under the knife visit your physiotherapist and see if they can’t provide a solution that works for you.
Andrew@PhysioPRO
BY:
Knee injuries / Lower Limb injuries

Patellar Dislocation
This unfortunate injury is associated with sports that involve repetitive running, jumping, or kicking such as soccer and rugby.
 The patella (kneecap) is a loose bone that sits in your quadriceps and patella tendons. It glides up and down a groove (the trochlea groove of the femoral condyle) as you bend and straighten your knee.
The patella (kneecap) is a loose bone that sits in your quadriceps and patella tendons. It glides up and down a groove (the trochlea groove of the femoral condyle) as you bend and straighten your knee.
Patellar dislocation occurs when the patella is displaced from this groove, most commonly laterally (towards the outside of the knee). This may either be caused by something traumatic especially where there is a history of a traumatic force to the kneecap or it can occur in the absence of trauma as is the case in young girls with associated ligamentous laxity
The stabiliser in your kneecap that protects against displacement is the medial patellofemoral ligament. Anatomically it acts as a passive check to prevent the patella from extreme lateral displacement which is why we find that in the majority of dislocation cases it is disrupted.
Patients usually complain of the knee suddenly giving way while jumping or running/twisting and the subsequent development of severe pain. A feeling of something “moving out of place” or “popping” is quite common. Often the dislocation reduces spontaneously with knee extension. But, swelling develops almost immediately.
It is common to mistake this injury for an Anterior Cruciate Ligament ( ACL) rupture as both conditions have similar mechanisms of injury with an audible “pop” and giving way of the leg as well as a quick development of swelling. But, on examination of a patellar dislocation there is usually gross swelling, marked tenderness over the medial (inside) border of the patella and when attempting to push the patella in a lateral direction the patient experiences pain or apprehension. Quadriceps muscle contraction aggravates the pain.
Most first-time dislocations are treated without surgery, with pain relief medication, immobilization of your knee with an extension splint for 2-3 weeks. During this time period you should be using crutches, and be following a rehabilitation program.
The most important aim of rehabilitation after such an injury is to reduce the chances of a recurrence. Hence the rehab program is lengthy and emphasizes core stability, vastus medialis obliquus strength, and stretching of the lateral structures when tight.
Surgery is indicated for second dislocations, or in patients not improving with appropriate rehabilitation (the re-dislocation rate after primary patellar dislocation managed non-operatively is anywhere between 15-44%). Medial patellofemoral surgery has become the surgery of choice.
So if you find yourself “buckled at the knees”, follow the RICE principle in the acute stage (Rest, Ice, Compression and Elevation) and seek treatment from your physiotherapist and/or orthopaedic doctor.
Andrew@PhysioPRO
BY:
General Health/Fitness / Knee injuries / Lower Limb injuries

Achilles Tendinopathy
The Achilles tendon is made up of the combined tendons of the gastrocnemius and soleus muscles (the two calf muscles). It is the thickest and strongest tendon in the body. But, that doesn’t make it immune to injury. Even the legendary Achilles – amongst the strongest and bravest Greek warriors – met his untimely demise following an injury to his Achilles tendon.
Injury to the Achilles tendon occurs when the load applied to the tendon exceeds the ability of the tendon to withstand that load. It is most common among males aged 30-50. These over-use Achilles tendon injuries may arise with increased training volume or intensity, change in training surface or footwear or decrease in recovery time between training session.
An athlete’s biomechanics might also predispose them to Achilles tendinopathies. These biomechanics include excessive pronation or supination of the foot (where the foot tends to fall inwards towards the arch or be pushed outwards), calf weakness and altered tibial or femoral mechanics etc.
Most of the time the athlete will notice a gradual development of symptoms, complaining of morning stiffness and pain, which diminishes with walking and application of heat. The two common sites of pain are the midportion of the Achilles tendon and the insertion of the Achilles tendon at the calcaneus.
One of the first things to look at when treating these problems is to identify and correct any predisposing factors i.e. training methods, footwear, orthotic and biomechanical correction.
Once these have been addressed the athlete should commence an eccentric training program, where they focus on controlling the negative motion of the repetition i.e. where the muscle is working in a lengthened state. The Alfredson painful heel-drop protocol for Achilles tendinopathy has shown to be very successful in treating midtendon Achilles pain. It consists of two main exercises – the ‘gastrocnemuis drop’(knee fully extended) and the “soleus drop”(knee bent to 45 degrees). Both exercises start on a step with the calf in a raised position. From this position the patient slowly lowers the heel so that the foot is parallel to the ground. Patients should do 3 sets of 15 repetitions twice daily for 12 weeks everyday of the week.

Patients should not be put off by the fact that the pain may worsen at the start of the program as this is part of the normal recovery process. If a patient experiences no pain during the exercises, they are advised to increase the load until the exercises provoke some pain i.e. add a weighted backpack. If you are suffering from pain at the insertion of the Achilles tendon then you should do a similar exercise program but remove the step, just do it standing on the floor, as this has been shown to be more effective.
With the correct treatment approach and the guidance of your physiotherapist, Achilles tendinopathy can be successfully managed and overcome.
Andrew@PhysioPRO
BY:
Ankle injuries / Foot injuries / Lower Limb injuries

A MUST-DO stretch
Now before you start panicking, NO, we are not going to be doing the stretch you see above, but we are going to show you a REALLY important stretch…
Most people are aware of the importance of stretching, and we have covered the topic on the benefits of stretching in an older post that you can read here, but what I would like to focus on today is the importance of stretching your HIP FLEXORS. As a Physiotherapist, I consider this muscle group to possibly be the most important muscle group to stretch, as it not only affects athletic ability but also your posture, and subsequently, chronic pain.


First for some anatomy. Your hip flexors are comprised of 3 distinct muscles namely: Iliacus, Psoas Major and Rectus Femoris (bet you probably never heard of them?).
Iliacus and Psoas Major (often grouped together and called Iliopsoas) are pure hip flexors (bringing your knee to your chest), whilst Rectus Femoris is a hip flexor and knee extensor (as it crosses both the hip and knee joint).
If you have a look at the first picture above (left), you will notice that the Psoas muscle is attached to the lower part of your spine. Thus, if it is tight, it actually pulls your spine down and exaggerates the curve of your lower back (anterior pelvic tilt). Together with the other two muscles being tight, this can account for “hyperlordosis” and lead to lower back problems and pain.

So why do they get so tight? Surely if you are not exercising these muscle, there is no reason for them to become overly tight?
There are two main causes for this. Firstly, we sit way too much, and secondly, we all like to have a six-pack, so if we do get a few minutes to exercise, we tend to do sit ups…
Now I’ve said it before, “Humans were just not designed to sit all day long!”, so for the majority of people that sit most of their day, these hip flexor muscles are in their shortened position for hours on end, and as a result, they become shortened and tight. Then when you do finally stand up, they are “fixed” in this position.
The second point was on sit ups and most other stomach exercises. Most people don’t realize this, but if you do a standard sit up (i.e. lying on your back, knees bent and then curling your back to bring your chest to your knees), your hip flexors are doing about 70% of the work…. Whether you bring your chest to your knees, or your knees to your chest, its the same movement– HIP FLEXION! (on a side note, thats the reason a lot of people get lower back pain when doing sit ups-tight hip flexors).
So here come the Rescue Remedy:
Its called many different names, but we like to call it the PROPOSAL STRETCH- for obvious reasons

I teach 2 different ways of doing this, either as you see above (more effective as you are bending the knee as well, so you are also stretching Rectus Femoris), or by placing your back leg on a chair (below). If you are doing it right, you should feel the stretch in the front of your hip, and possibly also slightly on the front of your thigh. People that do a lot of squatting movements (Crossfit, gym, skiing etc), or lunges (squash, tennis etc) would benefit immensely from this stretch, as It could limit your ability to get into those positions.

Hold this for 30 seconds and repeat for 3 sets, at least 2-3 times a day (more if you are sitting all day long).
Happy Stretching
Ric@PhysioPRO
BY: Riccardo Vaccaro
Back injuries / Hip injuries / Lower Limb injuries