

Modified Shoulder Stretches
Sometimes just by modifying the position or way you perform a stretch slightly, you can have much better results and outcomes. So when I came across an article about two modified shoulder stretches, I just had to share it with all of you.
Two of the most commonly used shoulder stretches to increase the flexibility of the posterior soft tissues are the cross-body and sleeper stretch exercises. But, based on the inability to stabilize the shoulder blade and control glenohumeral joint rotation with the cross-body stretch and the potential for subacromial impingement with the sleeper stretch, it has been recommend that modifications to both of these commonly performed stretches be made.
The modified sleeper stretch is performed with the athlete in a sidelying position, trunk rolled posteriorly 20° to 30°, and shoulder elevated to 90°. In this position, the athlete passively pushes his forearm down towards the bed using the opposite arm, a towel may also be placed under the arm of the stretched limb. This modified sleeper stretch position puts the posterior structures of the shoulder under more tension thus making it more effective.
 The cross-body stretch is often performed with the athlete in an upright standing position, using the opposite hand to horizontally adduct the targeted shoulder (pull your arm across your body).
The cross-body stretch is often performed with the athlete in an upright standing position, using the opposite hand to horizontally adduct the targeted shoulder (pull your arm across your body).
This method has the disadvantage of not providing stability to your shoulder blade and allows excessive external rotation of your shoulder. Due to this optimal stretch of the posterior shoulder is not achieved. Therefore, to better stabilize the shoulder blade, it has been suggested that the athlete be in a sidelying position, and, to restrict external rotation of the shoulder,the athlete should align the forearms together with the opposite forearm on top.

Well I hope these little adjustments to your stretching techniques yield large results.
Andrew@PhysioPRO
Reference: Journal of Orthopaedic & Sports Physical Therapy, 2013, Volume: 43 Issue: 12 Pages: 891-894
BY:
Shoulder injuries / Upper Limb injuries

Sorting out your Shoulder- Part 2
In my last article on sorting out the shoulder, I touched on the importance of scapula positioning in shoulder injuries. In today’s post, I will discuss the relevance of this to shoulder mechanics and some tips to resolve it.
The scapular plays a vital role in shoulder movement. Lets just say that if your scapular couldn’t move on your chest wall at all, you would have less than half of the movement in your shoulder as what you do right now.
With many people developing rounded shoulders and upper backs (as a result of poor posture, bad sitting habits and certain sports), the scapular position on the chest wall is compromised.
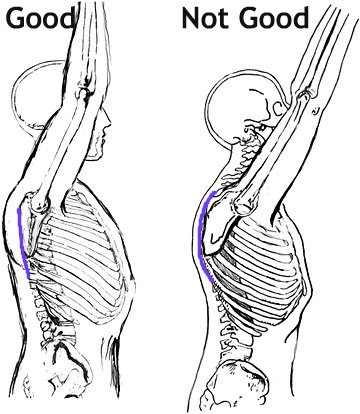
In these cases, the scapular tilts forwards and up (called protracted) and as a result, certain movements (especially overhead) become limited or painful. In addition, the stiff upper back further limits overhead movement and together, this can easily result in a condition called Impingement Syndrome, and/or lead to a rotator cuff tear.
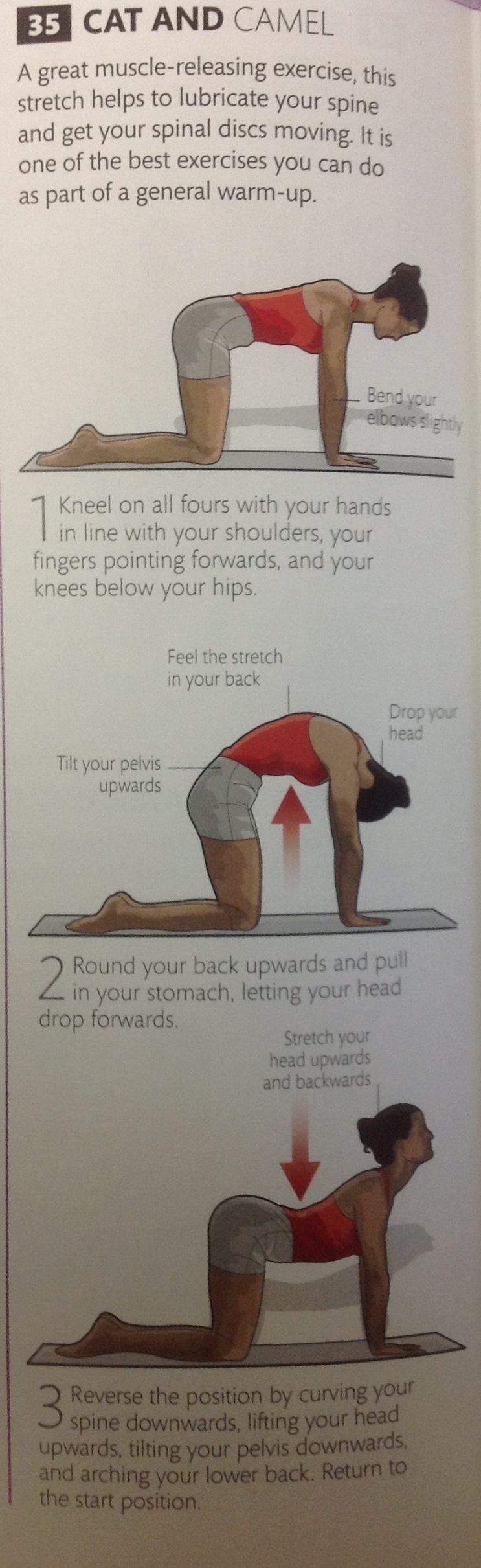
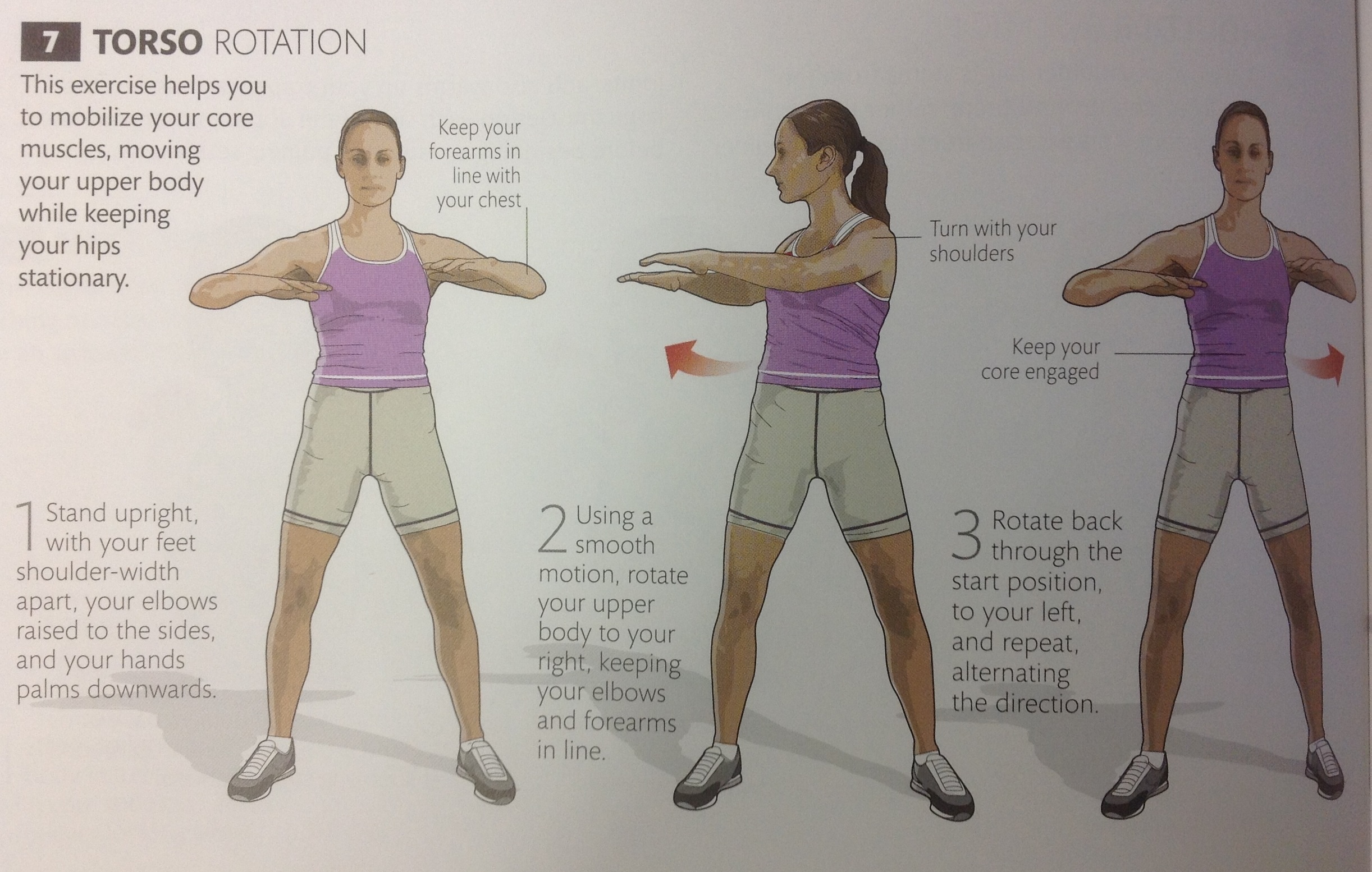
So the first trick is to loosen up or ” mobilize” the upper back.
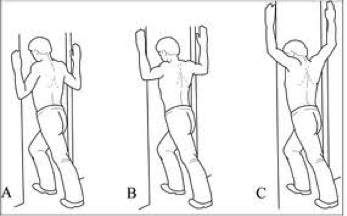
Below are 5 exercises to mobilize the thoracic spine.


Then we need to address scapular position. This can be tricky, because its not as simple as pulling your shoulders back together (Adduction). The movement is more of a small downward roll and is known as “setting the scapula”. If done correctly, the muscles between your shoulder blades SHOULD NOT WORK (Bottom right of pic below). Again, this is tricky, but once you have been shown it once it becomes simple.

So if you do any overhead sports or weight lifting (Crossfit athletes-this is a must) make sure you work on these two areas and it should help prevent future problems.
Good luck
Ric@PhysioPRO
BY: Riccardo Vaccaro
Shoulder injuries / Upper Limb injuries

Sorting out your Shoulder

Your shoulder joint is the most unstable joint in your body. If your hip joint is likened to a ball sitting in a socket, then your shoulder joint is likened to a golf ball sitting in a tee…its can slip out quite easily. This is because we need to be able to move our shoulders in a wide arc of movements (think bowling a ball, swinging from a branch or even just reaching to scratch your back), but this increased mobility comes at a price.

As a result of a very “shallow” joint surface, the muscles around your shoulder joint need to be very strong in order to hold the joint in place. These muscles are known as your ROTATOR CUFF, a group of 4 muscles, all working synergistically to hold the joint in place. From the picture below, you can see how they pretty much “pull” the ball of the humerus into the scapula.

The problem occurs when one of these Rotator cuff muscles get damaged, either through a sudden injury (like a tear) or through gradual overload (tendinosis). Because they all act as one unit, when as individual muscle is injured, the balance is upset and leads to further injury or loss of movement.
Another common Rotator cuff pathology is something called Impingement Syndrome. This is where the tendon of Supraspinatus becomes impinged or “pinched” in the groove it travels through. A major cause of this type of problem is as a result of poor posture. If the scapular is sitting more forward than it should (i.e. if you have rounded shoulders), the entire mechanics of how the shoulder joint moves is affected and can result in impingement.
Making sure your rotator cuff is strong and that your scapular sits in the correct position is half the battle won against treating AND preventing shoulder injuries.
So what do you need to do?
As you can imagine, being such a complicated joint, each individual needs to be given a specific set of exercises to improve shoulder stability and prevent injury. The basic process is STRETCH, STABILISE and STRENGTHEN.
Below is a general program that will assist most individuals:
STRETCH
 Hold each stretch 30 seconds
Hold each stretch 30 seconds
STABILISE
 Hold each position 10 times 10 seconds
Hold each position 10 times 10 seconds
STRENGTHEN
 Side lying external rotation 3 sets of 15 (1-5kg)
Side lying external rotation 3 sets of 15 (1-5kg)
 Can also be done in standing with a band (3 sets of 15-20)
Can also be done in standing with a band (3 sets of 15-20)
 Also done at 90 degrees for throwing athletes and weight-lifters
Also done at 90 degrees for throwing athletes and weight-lifters
Till next time, stay strong…
Ric@PhysioPRO
BY: Riccardo Vaccaro
Shoulder injuries / Upper Limb injuries

Aerobic vs Anaerobic Training
Training is the pursuit of any activity that will ultimately lead to an increase in performance in a specific sport. That’s what we mean when we talk about training!
So, training should be directed at bettering performance in an athlete’s chosen sport. As physiotherapists we should identify the most important components of fitness for each particular sport and tailor an athletes training toward improving these particular components.
Different training methods exist. These include aerobic training, anaerobic training, plyometric training, agility training, strength and power training – the list goes on. Today we are going to talk specifically about two of the most common types of training…. aerobic and anaerobic training.
Aerobic training or endurance training is performed to increase aerobic capacity or fitness. We measure aerobic capacity by measuring VO2 Max or the maximum oxygen an individual is able to utilize in one minute, per kilogram of body weight. VO2 Max can be measured in a fancy laboratory, but unfortunately most of us don’t train in this sort of setting, rather opting for the sports field or the gym. Luckily there is a simpler, albeit less exact method, known as predicted VO2 max which is estimated by measuring the heart rate at a specific workload which is a method commonly used.
It’s reported that aerobic training effects occur while maintaining a heart rate of between 70% and 85% of one’s maximum heart rate. Maximum heart rate is estimated by subtracting your age from 220. So it is pretty easy to do: for a 30 year old like me, max heart rate would be 220-30=190 beats per minute. And the ideal range of heart rate for me to produce an aerobic effect would be between 135 (70%) and 160 (85%) beats per minute.
And you thought jocks didn’t do maths!
Many sportspeople find benefit in the endurance and fitness gains made by training aerobically as well as the health benefits of a stronger cardiovascular system and resultant weight loss.
Anaerobic training burns glucose as an energy source but does this without oxygen present, to produce energy. Oxygen is absent because this sort of training is typically high intensity for a short period of time and there isn’t time for full oxygen delivery to the muscle cells using the glucose. This pathway utilizes ATP as its energy substrate. The process produces less energy per molecule of glucose utilized than aerobic exercise does when burning up that glucose with oxygen present.
Anaerobic training improves the capacity to maintain a high rate of power production at very high intensities for short period of time. This type of training helps maintain muscle recruitment and muscle contractile function after training so that the onset of fatigue is delayed, as well as improving the body’s tolerance to lactic acid build up. Lactic acid is a by-product of training anaerobically and contributes to the discomfort felt while training.
Interval training or intermittent exercise is the most efficient method of increasing anaerobic fitness. Such training involves bouts of exercise separated by periods of rest or recovery. The principle behind this type of training is to achieve a level of lactic acidosis with one individual effort and then allow the body to recover from its effects before embarking on another bout of exercise. This is done to train the body to cope with higher levels of lactic acid before shutting down and to recover faster.
As mentioned, to obtain maximum gains from interval training it must be activity/sport specific. Also remember that because of its increased intensity, the potential for injury is a little higher than that presented by aerobic training. It’s therefore beneficial for athletes to use a variety of training methods to take advantage of the benefits offered by each and allow time for rest and recovery of the body.
Andrew@PhysioPRO
BY:
General Health/Fitness / Lower Limb injuries / Upper Limb injuries

Hypermobility- a quick test to see which side of the spectrum you’re on
Our bodies are all different. Some are tall, some short, some big, some small and the same variety is found when it comes to the tissues within. Some people have more collagen in their ligaments and tendons which means they tend towards being more rigid and stiff. Others have less collagen and are far more flexible. As with most things in life, problems can occur on either extreme.
Let’s deal with one side of the spectrum – being very flexible or ‘hypermobile’. The problem here is that increased laxity or flexibility in the joints makes the joints more unstable and puts a person at a greater risk of injury, especially for those involved in contact sports. As we get older the body naturally stiffens up so hypermobile individuals that avoid injury early on in life are generally able to be more active older adults.
The Nine-Point Beighton Hypermobility Score is a quick and easy test to rate how hypermobile you are. It’s a simple 9 point system where the higher the score the higher the laxity. It is scored as follows:

Scoring high on the Beighton scale doesn’t necessarily mean you have Hypermobility syndrome as you could be hypermobile with no adverse symptoms (which include pain in the muscles and/or joints). Generally if you score either 4 or 5 out of 9 you are on the hypermobile end of the spectrum and should take precautions to prevent injury and work on stabilising and proprioceptive exercises, such as balancing on different surfaces while performing sports specific exercises, so that you can stay fit and healthy into your old age.
BY:
General Health/Fitness / Lower Limb injuries / Upper Limb injuries

Recovery Rules
With the Olympics currently in full swing, I’m sure many of you are enjoying all the top class sport showing on our televisions. Olympic athletes compete at the highest levels for consecutive days – sometimes even twice in the same day. How quickly and how well they RECOVER is vital for their optimal performance and could be the difference between going for Olympic gold and going home early.
The main aim of a post-game/event program is to enhance recovery, to maximize performance and minimize potential for injury at the next event. Recovery programmes have the following objectives:
- Restoration of function
- Neuromuscular recovery
- Tissue repair
- Resolution of muscle soreness
- Psychological recovery
A number of recovery methods are used by sportsmen and woman. Though there’s limited research in to the efficacy of most of them, let’s look at a few of the most popular techniques used:
Warm-down (active recovery)
Most athletes perform a warm-down of between 5 and 15 minutes after intense exercise followed by stretching of the muscles used in their specific sport. The warm down is also generally specific to the nature of their particular sport.
Cold Water Immersion (CWI)
 As the name suggests, players immerse themselves in ice baths ranging from 5-15°C for up to 5 minutes at a time. This has a cooling effect on the body tissues. CWI is associated with a peripheral vasoconstrictive response, reduced perfusion, and a decrease in oedema (which all help control the inflammatory response). However sportsmen with a history of cardiac problems such as arrhythmias should avoid CWI as it results in “cold shock” with associated increase in heart rate, blood pressure, respiratory minute volume, and metabolism, thus placing extra stress on the cardiac system.
As the name suggests, players immerse themselves in ice baths ranging from 5-15°C for up to 5 minutes at a time. This has a cooling effect on the body tissues. CWI is associated with a peripheral vasoconstrictive response, reduced perfusion, and a decrease in oedema (which all help control the inflammatory response). However sportsmen with a history of cardiac problems such as arrhythmias should avoid CWI as it results in “cold shock” with associated increase in heart rate, blood pressure, respiratory minute volume, and metabolism, thus placing extra stress on the cardiac system.
Massage
Intense training causes prolonged elevation of muscle tone in both resting and contracted states. This increased tone or “muscle tightness” limits the extensibility and shock absorbency of soft tissue and thus predisposes the tissue to strain. Active trigger points that result from heavy training may reduce muscle strength. All these problems can impair training and competition and can progress to injury if they are not resolved. Soft tissue therapy is thought to work by reducing excessive post-exercise muscle tone, increasing muscle range of motion, increasing the circulation and nutrition to damaged tissue, and deactivating symptomatic trigger points. It also helps to identify any soft tissue abnormalities, which if untreated could progress to injury.
Nutrition
Nutrition aids in the recovery from intense exercise by replenishing glycogen stores and providing necessary protein and water. Repetitive bouts of activity can cause profound glycogen depletion and substantial breakdown of muscle proteins which could lead to impaired sporting performance. Athletes are encouraged to consume a carbohydrate rich snack/meal that provides 1-1.2g of carbohydrate per kg of body weight as well as 10-20g of high-quality protein within the first hour post exercise, as this is when rates of glycogen synthesis are greatest. Glycogen is the major energy source for muscular activity in the body. Large amounts of fluid may be lost during exertion, especially with increased intensity and in hot conditions. Rehydration is vitally important to replace the lost fluid as well as electrolytes (especially sodium) lost through sweat.
Deep-water running
This recovery method involves running in the deep end of a swimming pool using a buoyancy vest. It is a form of cross-training that reduces the impact put on your joints and thus reduces overuse injuries.

Compression Garments
Lower limb tights and below-knee socks are advised for athletes soon after finishing their event. Athletes should leave them on for the next 24 hours. This aids in recovery from post-event muscle soreness.
Lifestyle factors such as adequate rest and sleep as well as the psychology of the athlete have also shown to influence recovery times.
As you can see what the athlete does off the track/field might be as important as what they do on it and coaches should be encouraged to incorporate recovery time into athletes’ schedules.
Andrew@PhysioPRO
BY:
General Health/Fitness / Lower Limb injuries / Upper Limb injuries

Tip of the WEEK
I thought I would just share a neat little trick that I teach most of my patients to manage their own muscular issues. Its so easy and effective that most of my patients end up saying ,”Why didn’t I think of that??”.
All you need is a wall or floor and a tennis ball….Place the tennis ball against the wall or floor (depending on the area you are treating) and then find that knot (trigger point) with the ball. Now apply pressure to the area using your body weight.

You want to apply a even steady pressure at first, till you feel a moderate ache and hold it there. You should feel it easing off after 30-45 seconds, so either push harder or find a new spot. If you feel up to it, you could even rub up-and-down or side-to-side over the ball to free up that tissue.
Whats so great about this technique is that YOU can decide how much pressure to apply and the ball never gets tired (unlike your partner). This also works great for loosening up stiff muscles after a heavy training session. Just make sure you are not doing this with an acute muscle tear (i.e. a “pulled” hamstring) as it could cause further damage.
So there you have it, your very own “physio” that fits in the palm of your hand and you can even take him on holiday with you…
Ric@PhysioPRO
BY: Riccardo Vaccaro
Back injuries / General Health/Fitness / Lower Limb injuries / Upper Limb injuries

Those ANNOYING things that mimic
Trigger points are hypersensitive areas within a muscle belly, commonly called “knots” that when stimulated, usually refers pain in areas around and away from the actual trigger point. They MIMIC pain in predictable band(s) away from the trigger point and also cause contractions in muscles that form taut bands… A trigger point is simply a small contraction within a muscle that can be excruciatingly painful.
Common ways in which trigger points mimic other conditions:
Weight-bearing on one leg more than the other (usually when we’ve had an injury to one side, we bear less weight on that side for example), can cause trigger points to develop in the gluteal muscles. Looking at this pain pattern, we could assume this to be sciatica. Sciatica is the description of a pain pattern and not a true diagnosis. (Fig.A below)

Another scary referral pattern is when a patient complains of severe pain in the left side of chest and down into the left arm. After appropriate testing for a possible heart problem is found to be negative, trigger points in the pectoral (chest) muscles are a likely cause for the chest and referred pain down into the arm. This pain referral pattern closely mimics that of a heart attack…and more often then not, they’re just as painful and stressful.
 Severe headaches have become all too common. More often than not, after conducting many scans and tests, the muscles in and around the neck and jaw are found to be harbouring trigger points that are causing the headaches. These muscles contract strongly and can compress nerves and blood vessels causing muscle and nerve pain.
Severe headaches have become all too common. More often than not, after conducting many scans and tests, the muscles in and around the neck and jaw are found to be harbouring trigger points that are causing the headaches. These muscles contract strongly and can compress nerves and blood vessels causing muscle and nerve pain.

Other severe presentations that may involve trigger points as their cause are the 6-pack abdominal muscles mimicking appendicitis and other abdominal pains.
A wide range of sports injuries including: Tennis Elbow, Shin Splints, Biceps Tendonitis and Bursitis, may involve muscles that mimic and these conditions.
There may be various causes that flare-up trigger points, these may include:
Long term or very sudden overuse of muscles, activation by other trigger points usually in neighbouring muscles, disease, psychological distress (via systemic inflammation), post-surgery, direct trauma to the region, when nerves do not function properly along their path (radiculopathy), infections and chronic health issues such as diabetes, arthritis, smoking, etc.
Common treatment modalities we would use at PhysioPRO to treat trigger points could include:
- Proper diagnoses of trigger points and appropriate referral if serious pathology is suspected.
- Myofascial release techniques and ischaemic pressure.
- Dry-needling.
- Muscle energy techniques.
- Posture correction, Strapping and Taping techniques.
- Proper muscle activation, muscle and movement re-education.
For thorough assessment and comprehensive treatment kindly contact us….
BY:
Back injuries / General Health/Fitness / Lower Limb injuries / Upper Limb injuries

Tender Tendons
I’m sure you’ve heard of the term “tendonitis” before, and you probably know of someone who has (or had) “tendonitis” of the elbow I.e. Tennis or Golfers’ elbow. Technically they are wrong, and it could be hampering their recovery!!
In actual fact, tendonitis is a very short lived and infrequent tendon condition. What they most likely have is actually TENDINOSIS, or otherwise known as a tendinopathy.
So what’s the big difference you ask? Well, medical terms that end in “itis” usually indicate inflammation and swelling, however in these tendon conditions, no inflammatory cells are present. This then has a direct impact on the way in which we treat the condition. So if you or your friend has tendinosis, taking anti-inflammatory medication is actually having no effect, and you may as well be taking Smarties instead…
If its not inflammation, then what is it exactly?
Without getting too technical, the substance that makes up tendons (collagen) is in a big tangled mess instead of a nice, neat and tight parallel bundles of fibers. There is also increased fluid around the fibers and lots of small, poor quality blood vessels. This can occur in various tendons, but the most commonly affected are those of the elbow (Golfers’ and Tennis Elbow), knee (Jumper’s knee), hip and ankle (Achilles Tendinosis).


So if you shouldn’t take anti-inflammatories, what should you do?
Tendinosis is usually as a result of repeated OVERloading of the tendon and therefore the CAUSE of your problem needs to be addressed. It could be as simple as a lack of rotation at the shoulder that could be causing your tennis elbow, or over-pronation at your ankle causing Achilles tendinopathy. Your physio should evaluate all likely factors and address these to prevent re-occurrence of your injury.
Where previously we were concerned not to inflame the tendon, treatment now focuses on actually CAUSING an inflammatory reaction, thus increasing blood supply and stimulating healing. Although painful, eccentric loading exercises are the “gold standard” of treatment to improve these conditions.
Nitric oxide donor patches and Shock wave therapy have some evidence to suggest they work, and a relatively new technique known as PRP (platelet rich plasma) injections (a topic we will discuss in future posts) are showing positive short term results at reducing pain and improving function.
I would highly recommend wearing a counterforce brace or getting strapped, as this will reducing the mechanical load on the tendon and alleviate pain.
One last thing you need to know. Tendon injuries usually take a long time to heal, especially if you’ve had it for months, so be prepared for some rehab and don’t wait till your pain is excruciating before you seek medical advice.
BY: Riccardo Vaccaro
Ankle injuries / Elbow injuries / Knee injuries / Lower Limb injuries / Shoulder injuries / Upper Limb injuries