

Shoes in Sport
Of late, many a client has passed through the door with injuries stemming from incorrect training shoes. Conditions such as: Shin splints, plantar fasciitis, tendinopathies, stress fractures and overuse syndromes may be as a result of the this…
Shoes play and important role in our lives as we wear them most of the time is our daily activities. But how do I know what the right shoe is for my sport?
This is a quick go-to when having a look at which shoe is best suited for you.
Firstly you need to purchase a shoe that is in line with the activity you are performing.
Walking shoes: lightweight, with extra shock absorption in the heel and under the ball of the foot to decrease heel pain and burning/tenderness in the ball of the foot. Walking shoes are more rigid in the frontal area of the shoe for toe roll off. If you feel that you need more even weight distribution, a smoother transition from heel-to-toe and less force over the foot, look for a shoe that has a slightly more rounded sole.
Running shoes: have good overall shock absorption, and heel control. Check your running style first, as a heel-striker requires different shoes to a fore-foot/mid-foot striker!
Aerobic conditioning shoes: lightweight with extra shock absorption in the ball of the foot to prevent foot fatigue.
Tennis and netball shoes: give upper support with quick transferring of weight and side to side movements and a flexible sole for quick changes of direction. When playing on soft surfaces look for a softer sole shoe, and vice versa with a hard surface.
Basketball shoes: have a stiff, thick sole for more stability whilst on court. The high top gives extra ankle support but won’t prevent the risk of ankle injuries.
Cross training shoes: a combination of many features and therefore help you participate in more than one sport, without having to purchase more than one pair of shoes. It will be flexible in the forefoot for running and have lateral control for aerobics and court activities. Obviously, because they are the “jack of all trades” when it comes to functionality, they are not particularly good at any one specific component. For exmple, a cross training shoe shouldnt be worn to run more than 10km. Rather get a dedicated running shoe for that purpose.

How to go about choosing the correct shoe.
-Like clothes- different brands fit differently, so don’t take it for granted that if in the one brand you are a size 7 you would be the same in the next brand.
-Measure both feet when they are at their largest- usually after exercise or at the end of the day. Remember one foot may be larger than the other.
-Use the same type of sock that you would usually use in your activity of preference.
-Comfort is key- the shoe should mimic the shape of your foot
-There is an old saying- “the shoe will become flexible/ loosen with time” this is partially true, however when purchasing a shoe, you should not keep this in the back of your mind. The shoe should be comfortable and fit correctly when purchasing it!
-The widest part of your foot should not feel cramped in the shoe, you should be able to wiggle/ move your toes freely
-The part where your toes are in the shoe (toe box) should have enough depth to prevent chafing, or calluses formation
-Stand and ensure that there is about half the width of your finger between the big toe and the second toe.
-Test the shoe, walk around in it, and ensure that it is comfortable with no chafing. Your heel should not slide forwards and backwards either.
 Some extra tips
Some extra tips
If you participate in a particular sport 3 or more times a week, then a sport-specific shoe is advised.
Shoes need to be replaced depending on how often they are used and age. It is recommended that after 300 hours of aerobic activity, or a maximum of 800km have been reached on the shoes, they have run their course and need to be replaced, much like the tyres on your vehicle. Rubber degrades with age, so a shoe that’s more than 5 years old, regardless of mileage/hours still needs replacing!
These are just a few pointers in helping you find the right fit for your foot. So the next time you head out to upgrade your footwear to what your feet deserve, stop and think before you just choose a brand and type of shoe because of its aesthetic appearance. Choose FUNCTION over FASHION!
Happy shoe shopping!
Amy@physiopro
BY:
Ankle injuries / Foot injuries / General Health/Fitness

Acute injuries- RICE or MEAT?
Things are constantly evolving in the world of sports medicine. With a better understanding of how the human body works, comes an ever changing understanding of how best to treat it. One such notion which needs to be challenged is the age old acronym of R.I.C.E (Rest, Ice, Compress, Elevate) used for the management of acute injuries.

The “Rest” part of this strategy may in fact cause delayed healing and muscle atrophy. Several studies that have compared early PAIN-FREE movement to complete rest have shown decreased healing times and improved pain.
As I stated above, what is quite important is to start moving early on, but specifically without pain. Even some serious injuries/operations should allow for a degree of movement that is pain free.

Another area of uncertainty is the application of “ICE”. Whilst there is evidence that ice causes a numbing effect on tissue (by decreasing the speed and transmission of nerves), thereby reducing pain, the notion that icing decreases the inflammatory response and speeds up healing is being challenged.
Some studies are showing that the application of early ice (for 20 minutes in the acute stage of an injury) may in fact reduce the healing potential of tissue, and cause longer term negative effects on the healing collagen. So if your intention is to reduce pain, then ice may be appropriate, but if you think you are assisting the body healing process, think again…

What is now being suggested is a new acronym – M.E.A.T
MOVEMENT – as discussed earlier, must be pain-free
EXERCISE – the correct exercises done early on have been shown to reduce muscle wasting and improve outcomes
ANALGESICS – used to control acute pain, but be careful not to “mask” the pain so you can go back to activity too quickly. Again, avoid anti-inflammatories at first.
TREATMENT – from a Physiotherapist or other sports medicine practitioner. We can use other modalities to improve circulation and assist healing.
The Editor in Chief of The Physician and Sports Medicine Journal was quoted as saying,”Do you honestly believe that your body’s natural inflammatory response is a mistake?” I’ve said it in my article on anti-inflammatories, the first stage of healing is INFLAMMATION, but it seems we have all been hell-bent on trying to stop this.
It would appear that the more we learn about how to heal the human body, the more we realise it does a pretty good job, all on its own!
Ric@PhysioPRO
BY: Riccardo Vaccaro
Ankle injuries / General Health/Fitness / Knee injuries

We will, we will SHOCK you!!
Shock wave therapy (also known as extracorporeal shock wave) is a cutting edge form of treatment in the world of sports medicine. Its a very similar technology to that used to “blast” kidney and gallstones, and does not involve electrical shocks (don’t panic, this isn’t the dark ages) but rather mechanical pulses, similar to sound waves.
Although the physiological mechanism of how exactly this mechanical pulse works is still not fully understood, the research shows us that the “waves” cause microtrauma and inflammation, stimulating the formation of new blood vessels and nerve cells, and speeding up healing of tissue. There is also a positive effect on reducing pain through a pain gate mechanism.
In other words, it improves blood supply and speeds up tissue regeneration!
So why is this so amazing you ask?
Well basically its taking something the body would normally do on its own, and speeds it up significantly, without the need for injections or surgery. Numerous medical research reports have shown that shockwave therapy can be 80-90% effective at completely and rapidly resolving injuries within 3-6 applications.
The most significant application in sports medicine is in the treatment of chronic tendon, muscle and joint conditions. So things like:
- Tennis elbow/ Golfers elbow
- Rotator cuff tendinopathy
- Frozen Shoulder
- Trochanteric Bursitis
- Hamstring tendinopathy
- Achilles tendinpathy
- Patella tendinopathy
- Plantar fasciitis
- Muscle knots and trigger points
- ITB friction syndrome
- Chronic ligament pain
- And even more conditions are healing in weeks instead of months…
It is particularly effective in breaking down the calcification of tendons, commonly seen in the shoulders, as can be seen in the x-rays below…

As technology and techniques improve, so will we find new uses for shock wave therapy. In fact, I chatted to a Doctor at one of the top SA rugby teams, who said they use shock wave to treat nearly all injuries on their players and are getting fantastic results.
Already studies show that in bone fractures that either wont heal quickly, or at all, the application of a single shock wave treatment was effective in causing fracture healing in 87% of patients.
It also has applications in the healing of diabetic foot ulcers, treating cardiac chest pain and erectile dysfunction…but don’t come to me for that!
So if you, or anyone you know has one of the above conditions, give us a call to see if Shock Wave Therapy might be the treatment for you…
Ric@PhysioPRO
BY: Riccardo Vaccaro
Ankle injuries / Elbow injuries / General Health/Fitness / Knee injuries / Shoulder injuries

The DRUG called Exercise
The wonder drug called… exercise!
Imagine there was a drug you could take that did the following:
- Reduce heart disease by 40%
- Reduce your risk of stroke by 27%
- Decreased diabetes by 50%
- Decreases high blood pressure by 50%
- Lowers deaths and the risk of recurrent breast cancer by 50%, colon cancer by 60%
- Lowers the risk of Alzheimer’s disease by 33%
- Treat depression as effectively as Prozac or other behavioral therapies
Unfortunately there is no pill that can do all these (wishful thinking), but there is a drug out there that can, and it’s called Exercise!!
I recently attended a course by the “Exercise is Medicine South Africa” institute to discuss this very topic of EXERCISE being prescribed as a MEDICINE to all people. It’s part of a global initiative of the American College of Sports Medicine to promote exercise in a safe and effective way.
As with most of the population, most of my patients are aware of the importance of exercise. Those that don’t exercise regularly will always sheepishly admit that they know they should be exercising, but usually blame a lack of time or tiredness as their reason for not doing so.

Here are a few interesting things I picked up from this course:
- Not exercising for ONE day has the same health detriments as smoking THREE cigarettes!!!
As a non-smoker who chooses not to smoke due to the health implications, this came as a big surprise to me and puts into perspective just how damaging it is to be physically inactive.
- Its better to be FAT-AND-FIT than SKINNY-AND-UNFIT
Thats right! Just because you are not overweight doesn’t mean you are healthy.
- If you are not doing at least 150 minutes of exercise per week, you are considered high risk for developing a variety of health issues!!
That basically boils down to getting 30 minutes of exercise for 5 days per week. Less than that and you chances of mortality are more than someone who is obese, or smokes, or has diabetes.
- Being physically active during the day does not count as EXERCISE.
A lot of people believe that they get enough “exercise” by being on their feet all day or climbing a few flights of stairs during their day. The truth is, if your heart rate is not reaching between 50-70% of its maximum capacity for a minimum of 30 minutes (continuously) per day, you can’t say you are exercising.
Work that out quickly for yourself- take 220 and minus your age to get a rough idea of your Heart Rate (HR) max.
Then take your number, and multiply it by 0.5 to get 50% and 0.7 to get 70%.
So for a 35 year old that would be 220-35=185
185X0.5 =92.5 185X0.7=129.5
So this guy or girl would need to have their HR at between 92.5 and 129.5 beats per minute for 30 minutes a day.
On average, a brisk walk would get you into this target heart rate but as with all DRUGS, there are certain risk factors (especially for people who already have pre-existing medical conditions) so this is where Exercise is Medicine South Africa are working with health professionals in order to safely and efficiently prescribe exercise to individuals.
After an initial screening procedure, you would be grouped into either low, moderate or high risk, and your exercise program specifically tailored to suit your risk and needs.
One last thought…
There are 1440 minutes in a day. Can you really not find the time to use 30 of them towards living a longer life???
Ric@PhysioPRO
![]()
BY: Riccardo Vaccaro
General Health/Fitness

Practical Tips for a diabetic patient starting a physical activity program
There are two types of diabetes … Type 1 “juvenile-onset diabetes” and Type 2 “adult-onset” diabetes, both are characterized by diminished insulin secretion in the body resulting in increased blood glucose levels. Type 2 diabetes is a lot more common and as most of you could guess the onset of the disease occurs later in life compared to Type 1 diabetes.
For both Types though exercise and physical activity are highly recommended, but firstly it is very important that prior to any exercise a full assessment by a healthcare professional be performed to identify any possible risks associated with diabetes while exercising.
A combination of aerobic and resistance exercises provides the most benefit to those with diabetes. You should aim to do a minimum of 150 minutes per week of aerobic exercise spread over 3 days such as biking, walking, swimming, hiking etc .
Resistance exercise 2-3 times a week has been proven to improve insulin sensitivity and help control glucose levels in the body. It is also very important to always monitor blood glucose levels before, during and immediately after exercise.
Here are some Nutritional advice while exercising
- Exercise 1-2 hours after eating a meal to ensure ideal glucose levels during exercise.
- Staying Hydrated before, during and after exercise is very important as dehydration can be confused with hypoglycemia.
- Fast- acting carbohydrates should be easily accessible during and immediately after exercise.
Some signs of hypoglycemia and things to be wary of
- Headaches
- Excessive sweating
- Confusion
- Nervousness
- Tremors
- Hunger
- Convulsions
And just to end of this article here is a short list of items you should always have with you while exercising
- Insulin medication
- Fast- digesting carbohydrates
- Medical Id bracelet
- Water
- Glucose monitor
- Comfortable shoes and socks
Andrew@PhysioPRO
BY:
General Health/Fitness

Take this pill-tear that muscle!
So you go to see your doctor because you have the flu. The doctor books you off and prescribes antibiotics. One or two weeks later you start to feel better so you decide to go for a jog, and thats when it happens! Suddenly you hear a loud “crack” and start limping. You’ve TORN your achilles tendon and you weren’t even straining yourself?
This same scenario has happened to many people and its not because they were sick or unfit, its because of the ANTIBIOTIC that was prescribed!!!
A group of Antibiotics called Flouroquinolones are associated with a wide variety of musculoskeletal problems that affect muscle, tendon, bone and cartilage. They are commonly used to treat a variety of urinary tract, digestive, respiratory and skin infections amongst others. In the USA, this class of antibiotic is THE most prescribed type to adults, even though since as early as 1983 it was known that this drug was toxic to musculoskeletal tissue. Symptoms have been known to occur as early as 2 hours after the initial dosage and as late as 6 months after!!
In one study of 42 patients who developed Tendon related problems, 76% experienced tendinopathy (sick tendons) and the other 24% had complete ruptures of the tendon. Muscle symptoms range from mild muscular pain to a very serious and life threatening condition known as Rhabdomyolysis. Bone problems are less conclusive in humans, but in animal studies, it has been shown to slow down or even stop a bone from repairing itself.
What they have discover in more recent times is that there are factors which make you more at risk of developing these symptoms. These include: increasing age, use of cortisone, playing sport, a previous history of tendon or joint problems, magnesium deficiency and diabetes to name but a few.
So what should you do or how can this be avoided?
Not to discredit any Doctor or other health professional, but if you are being prescribed an anti-biotic, check with them that this will be safe to use, especially if you are a physically active person. I had a patient recently that developed general muscle ache, along with severe elbow pain for no apparent reason. She had all the symptoms of someone that had trained heavily the past few days, which she hadn’t. She also had Tennis elbow symptoms and it turned out she was prescribed a Flouroquinolone by her dentist for a tooth infection the week before…
So your doctor should get a thorough history of your previous musculoskeletal problems, find out about your activity levels, ask about associated risk factors and advise you to stop the drug immediately if it is causing any symptoms.
If you are an Athlete, you should definitely not be using this class of antibiotic unless there is no available alternative drug. If you are presently taking this drug, or have used it in the past 6 months, reduce your training intensity, avoid ballistic movements and be aware of any development of symptoms.
Ric@PhysioPRO
Full article by Hall et al. Published in the American Academy of Physical Medicine and Rehabilitation, Vol 3. 132-142, Feb 2011.
BY: Riccardo Vaccaro
General Health/Fitness

Balance is the key
Ankle injury is arguably the most common sport injury. I tend to see a lot of patients coming into the practice complaining of repetitively “twisting “ their ankles. They will frustratingly announce ”that’s my bad ankle…I’m always twisting it” upset that they can’t seem to shake off the injury.
 Most of the time the reason for these continuous ankle problems, is a history of inadequate rehabilitation, especially in the aspect of balance and proprioception. Proprioception being the sense of knowing where a body part is in space, which is commonly lost after spraining an ankle. So if this is not properly re-taught, the patient is more likely to re-injure that same ankle when they return to sport.
Most of the time the reason for these continuous ankle problems, is a history of inadequate rehabilitation, especially in the aspect of balance and proprioception. Proprioception being the sense of knowing where a body part is in space, which is commonly lost after spraining an ankle. So if this is not properly re-taught, the patient is more likely to re-injure that same ankle when they return to sport.
In the initial returning to sport phase ankle braces and strapping can be used to add additional support as well as aid in proprioception of the ankle.
Exercises such as standing on one leg and trying to balance, progressing to closing your eyes while standing on the injured leg as well as standing on an unstable surface such as a balance board will all help improve your proprioception and balance.

Once you are comfortable with these more basic exercises you can now progress to more sport specific balance exercise. Focusing on keeping your balance while performing movements’ specific to your sport, the exercises are limitless.
The problem being most patients, once the pain is gone, stop there and don’t continue with the full rehabilitation program. So if you want to prevent those recurring nagging ankle injuries remember balance is the key.
Andrew@PhysioPRO
BY:
Ankle injuries / Foot injuries / General Health/Fitness / Lower Limb injuries

The Science of SCARS
Scars are our bodies natural “glue”. They form in wounds to try to weld together the damaged tissue, thus allowing us to function again. Collagen type 1 (the building material for every scar) is the chameleon of the cellular world. It is able to mimic the surrounding cells and tries to form a scar that is as similar in its properties as that of the parent tissue.
In the ideal world, these scars form perfectly and require no attention, however this is not always the case. Our jobs as Physiotherapists are to provide the optimal environment for the formation of scars, and the necessary treatment so that they allow for full, functional movements.
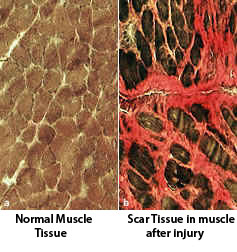
Lets take the example of a hamstring tear: When we tear a muscle, we damage muscle cells (fibers). These damaged cells do not regenerate themselves (you don’t form new muscle cells), you merely glue the tear up with collagen.
At first this collagen is delicate and fragile, but as it matures, it becomes thicker and stronger. It needs to become as strong as the rest of the hamstrings, so it can take load through it, but at the same time, it needs to be able to stretch so that it doesn’t tear again.
Start training too early and you tear the newly forming collagen, so the body lays down more collagen to try fix it and you end up with a thick scar that limits movement. On the flip side, if you delay putting load through the scar for too long (stretching or exercise), the scar will be “disorganized” and weak, and could re-tear.
The second problem with scars is that they can also “glue” together 2 different types of tissue. So getting back to the hamstring tear, when you tear the muscle, you most likely also damage the surrounding fascia. This thick “mesh” like tissue covers individual muscles and groups of muscles too. If the new scar welds together the muscle and the surrounding fascia, it will restrict the entire movement of that area, and can often affect the joint (e.g.knee).
This applies even more so when the skin has also been damaged (as in the case of a knife wound or surgery), as there are now multiple-layers of tissue that can become welded together. Occasionally we also see that nerves become “trapped” in scars and this further complicates matters.
So, in summary, the timing of therapy to the scar and the ability of you therapist to distinguish which structures are affected will greatly improve your outcome after injury. If only someone had told poor Harry Potter…
Happy Healing
Ric@PhysioPRO
BY: Riccardo Vaccaro
General Health/Fitness

Patellar Dislocation
This unfortunate injury is associated with sports that involve repetitive running, jumping, or kicking such as soccer and rugby.
 The patella (kneecap) is a loose bone that sits in your quadriceps and patella tendons. It glides up and down a groove (the trochlea groove of the femoral condyle) as you bend and straighten your knee.
The patella (kneecap) is a loose bone that sits in your quadriceps and patella tendons. It glides up and down a groove (the trochlea groove of the femoral condyle) as you bend and straighten your knee.
Patellar dislocation occurs when the patella is displaced from this groove, most commonly laterally (towards the outside of the knee). This may either be caused by something traumatic especially where there is a history of a traumatic force to the kneecap or it can occur in the absence of trauma as is the case in young girls with associated ligamentous laxity
The stabiliser in your kneecap that protects against displacement is the medial patellofemoral ligament. Anatomically it acts as a passive check to prevent the patella from extreme lateral displacement which is why we find that in the majority of dislocation cases it is disrupted.
Patients usually complain of the knee suddenly giving way while jumping or running/twisting and the subsequent development of severe pain. A feeling of something “moving out of place” or “popping” is quite common. Often the dislocation reduces spontaneously with knee extension. But, swelling develops almost immediately.
It is common to mistake this injury for an Anterior Cruciate Ligament ( ACL) rupture as both conditions have similar mechanisms of injury with an audible “pop” and giving way of the leg as well as a quick development of swelling. But, on examination of a patellar dislocation there is usually gross swelling, marked tenderness over the medial (inside) border of the patella and when attempting to push the patella in a lateral direction the patient experiences pain or apprehension. Quadriceps muscle contraction aggravates the pain.
Most first-time dislocations are treated without surgery, with pain relief medication, immobilization of your knee with an extension splint for 2-3 weeks. During this time period you should be using crutches, and be following a rehabilitation program.
The most important aim of rehabilitation after such an injury is to reduce the chances of a recurrence. Hence the rehab program is lengthy and emphasizes core stability, vastus medialis obliquus strength, and stretching of the lateral structures when tight.
Surgery is indicated for second dislocations, or in patients not improving with appropriate rehabilitation (the re-dislocation rate after primary patellar dislocation managed non-operatively is anywhere between 15-44%). Medial patellofemoral surgery has become the surgery of choice.
So if you find yourself “buckled at the knees”, follow the RICE principle in the acute stage (Rest, Ice, Compression and Elevation) and seek treatment from your physiotherapist and/or orthopaedic doctor.
Andrew@PhysioPRO
BY:
General Health/Fitness / Knee injuries / Lower Limb injuries