

We will, we will SHOCK you!!
Shock wave therapy (also known as extracorporeal shock wave) is a cutting edge form of treatment in the world of sports medicine. Its a very similar technology to that used to “blast” kidney and gallstones, and does not involve electrical shocks (don’t panic, this isn’t the dark ages) but rather mechanical pulses, similar to sound waves.
Although the physiological mechanism of how exactly this mechanical pulse works is still not fully understood, the research shows us that the “waves” cause microtrauma and inflammation, stimulating the formation of new blood vessels and nerve cells, and speeding up healing of tissue. There is also a positive effect on reducing pain through a pain gate mechanism.
In other words, it improves blood supply and speeds up tissue regeneration!
So why is this so amazing you ask?
Well basically its taking something the body would normally do on its own, and speeds it up significantly, without the need for injections or surgery. Numerous medical research reports have shown that shockwave therapy can be 80-90% effective at completely and rapidly resolving injuries within 3-6 applications.
The most significant application in sports medicine is in the treatment of chronic tendon, muscle and joint conditions. So things like:
- Tennis elbow/ Golfers elbow
- Rotator cuff tendinopathy
- Frozen Shoulder
- Trochanteric Bursitis
- Hamstring tendinopathy
- Achilles tendinpathy
- Patella tendinopathy
- Plantar fasciitis
- Muscle knots and trigger points
- ITB friction syndrome
- Chronic ligament pain
- And even more conditions are healing in weeks instead of months…
It is particularly effective in breaking down the calcification of tendons, commonly seen in the shoulders, as can be seen in the x-rays below…

As technology and techniques improve, so will we find new uses for shock wave therapy. In fact, I chatted to a Doctor at one of the top SA rugby teams, who said they use shock wave to treat nearly all injuries on their players and are getting fantastic results.
Already studies show that in bone fractures that either wont heal quickly, or at all, the application of a single shock wave treatment was effective in causing fracture healing in 87% of patients.
It also has applications in the healing of diabetic foot ulcers, treating cardiac chest pain and erectile dysfunction…but don’t come to me for that!
So if you, or anyone you know has one of the above conditions, give us a call to see if Shock Wave Therapy might be the treatment for you…
Ric@PhysioPRO
BY: Riccardo Vaccaro
Ankle injuries / Elbow injuries / General Health/Fitness / Knee injuries / Shoulder injuries

Modified Shoulder Stretches
Sometimes just by modifying the position or way you perform a stretch slightly, you can have much better results and outcomes. So when I came across an article about two modified shoulder stretches, I just had to share it with all of you.
Two of the most commonly used shoulder stretches to increase the flexibility of the posterior soft tissues are the cross-body and sleeper stretch exercises. But, based on the inability to stabilize the shoulder blade and control glenohumeral joint rotation with the cross-body stretch and the potential for subacromial impingement with the sleeper stretch, it has been recommend that modifications to both of these commonly performed stretches be made.
The modified sleeper stretch is performed with the athlete in a sidelying position, trunk rolled posteriorly 20° to 30°, and shoulder elevated to 90°. In this position, the athlete passively pushes his forearm down towards the bed using the opposite arm, a towel may also be placed under the arm of the stretched limb. This modified sleeper stretch position puts the posterior structures of the shoulder under more tension thus making it more effective.
 The cross-body stretch is often performed with the athlete in an upright standing position, using the opposite hand to horizontally adduct the targeted shoulder (pull your arm across your body).
The cross-body stretch is often performed with the athlete in an upright standing position, using the opposite hand to horizontally adduct the targeted shoulder (pull your arm across your body).
This method has the disadvantage of not providing stability to your shoulder blade and allows excessive external rotation of your shoulder. Due to this optimal stretch of the posterior shoulder is not achieved. Therefore, to better stabilize the shoulder blade, it has been suggested that the athlete be in a sidelying position, and, to restrict external rotation of the shoulder,the athlete should align the forearms together with the opposite forearm on top.

Well I hope these little adjustments to your stretching techniques yield large results.
Andrew@PhysioPRO
Reference: Journal of Orthopaedic & Sports Physical Therapy, 2013, Volume: 43 Issue: 12 Pages: 891-894
BY:
Shoulder injuries / Upper Limb injuries

Sorting out your Shoulder- Part 2
In my last article on sorting out the shoulder, I touched on the importance of scapula positioning in shoulder injuries. In today’s post, I will discuss the relevance of this to shoulder mechanics and some tips to resolve it.
The scapular plays a vital role in shoulder movement. Lets just say that if your scapular couldn’t move on your chest wall at all, you would have less than half of the movement in your shoulder as what you do right now.
With many people developing rounded shoulders and upper backs (as a result of poor posture, bad sitting habits and certain sports), the scapular position on the chest wall is compromised.
In these cases, the scapular tilts forwards and up (called protracted) and as a result, certain movements (especially overhead) become limited or painful. In addition, the stiff upper back further limits overhead movement and together, this can easily result in a condition called Impingement Syndrome, and/or lead to a rotator cuff tear.
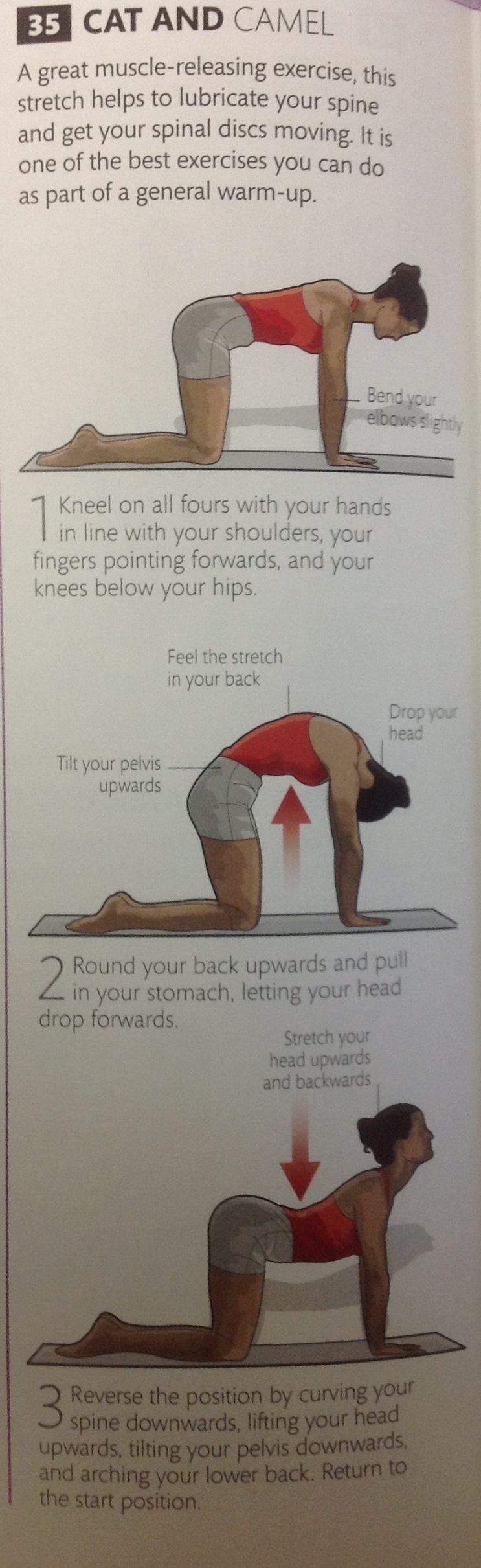
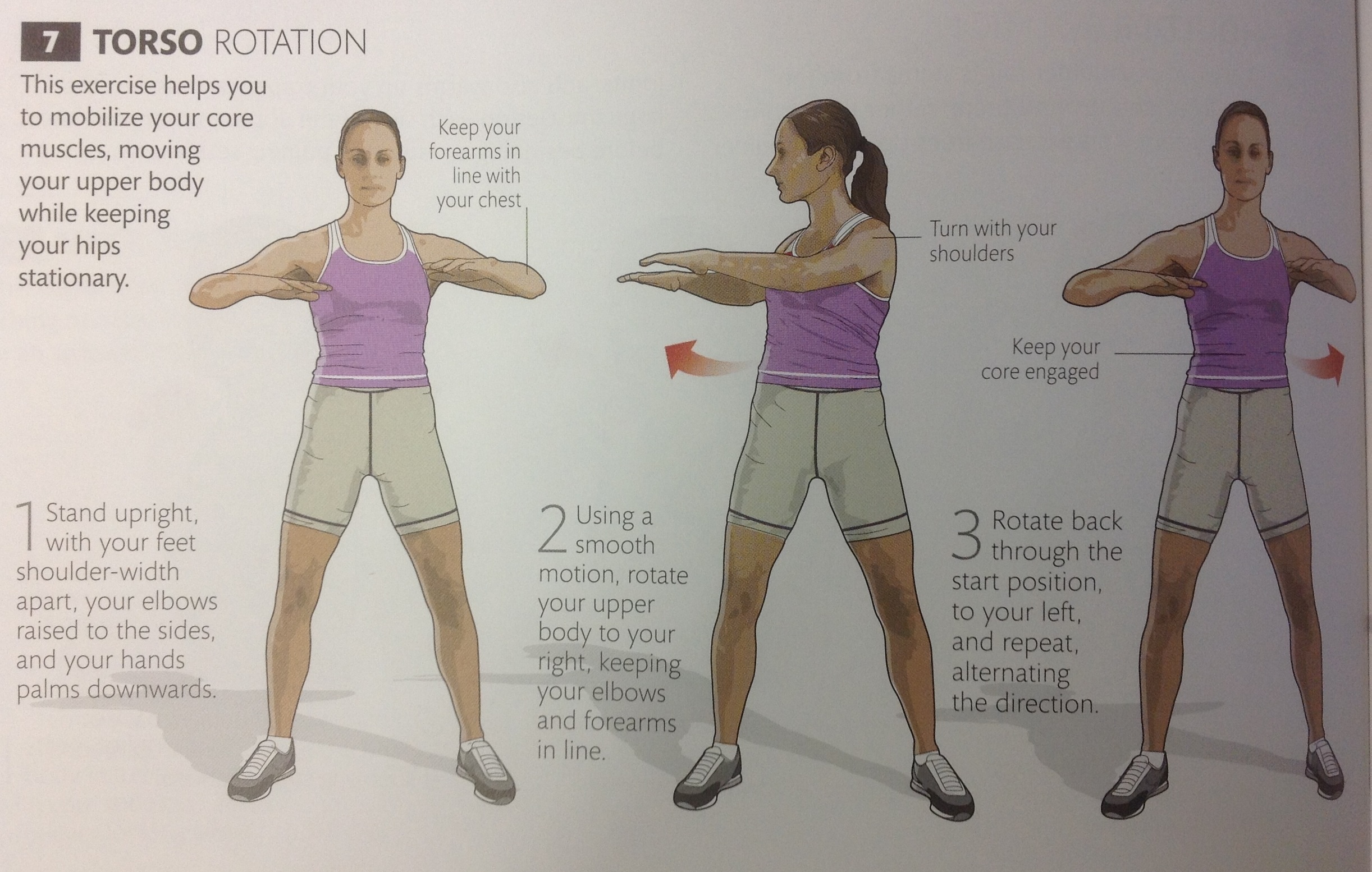
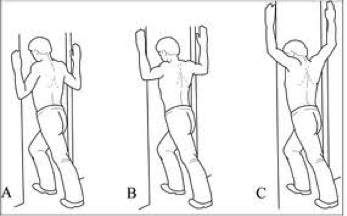
So the first trick is to loosen up or ” mobilize” the upper back.
Below are 5 exercises to mobilize the thoracic spine.


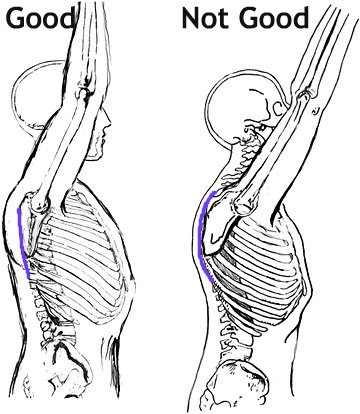
Then we need to address scapular position. This can be tricky, because its not as simple as pulling your shoulders back together (Adduction). The movement is more of a small downward roll and is known as “setting the scapula”. If done correctly, the muscles between your shoulder blades SHOULD NOT WORK (Bottom right of pic below). Again, this is tricky, but once you have been shown it once it becomes simple.

So if you do any overhead sports or weight lifting (Crossfit athletes-this is a must) make sure you work on these two areas and it should help prevent future problems.
Good luck
Ric@PhysioPRO
BY: Riccardo Vaccaro
Shoulder injuries / Upper Limb injuries

Sorting out your Shoulder

Your shoulder joint is the most unstable joint in your body. If your hip joint is likened to a ball sitting in a socket, then your shoulder joint is likened to a golf ball sitting in a tee…its can slip out quite easily. This is because we need to be able to move our shoulders in a wide arc of movements (think bowling a ball, swinging from a branch or even just reaching to scratch your back), but this increased mobility comes at a price.

As a result of a very “shallow” joint surface, the muscles around your shoulder joint need to be very strong in order to hold the joint in place. These muscles are known as your ROTATOR CUFF, a group of 4 muscles, all working synergistically to hold the joint in place. From the picture below, you can see how they pretty much “pull” the ball of the humerus into the scapula.

The problem occurs when one of these Rotator cuff muscles get damaged, either through a sudden injury (like a tear) or through gradual overload (tendinosis). Because they all act as one unit, when as individual muscle is injured, the balance is upset and leads to further injury or loss of movement.
Another common Rotator cuff pathology is something called Impingement Syndrome. This is where the tendon of Supraspinatus becomes impinged or “pinched” in the groove it travels through. A major cause of this type of problem is as a result of poor posture. If the scapular is sitting more forward than it should (i.e. if you have rounded shoulders), the entire mechanics of how the shoulder joint moves is affected and can result in impingement.
Making sure your rotator cuff is strong and that your scapular sits in the correct position is half the battle won against treating AND preventing shoulder injuries.
So what do you need to do?
As you can imagine, being such a complicated joint, each individual needs to be given a specific set of exercises to improve shoulder stability and prevent injury. The basic process is STRETCH, STABILISE and STRENGTHEN.
Below is a general program that will assist most individuals:
STRETCH
 Hold each stretch 30 seconds
Hold each stretch 30 seconds
STABILISE
 Hold each position 10 times 10 seconds
Hold each position 10 times 10 seconds
STRENGTHEN
 Side lying external rotation 3 sets of 15 (1-5kg)
Side lying external rotation 3 sets of 15 (1-5kg)
 Can also be done in standing with a band (3 sets of 15-20)
Can also be done in standing with a band (3 sets of 15-20)
 Also done at 90 degrees for throwing athletes and weight-lifters
Also done at 90 degrees for throwing athletes and weight-lifters
Till next time, stay strong…
Ric@PhysioPRO
BY: Riccardo Vaccaro
Shoulder injuries / Upper Limb injuries

Tender Tendons
I’m sure you’ve heard of the term “tendonitis” before, and you probably know of someone who has (or had) “tendonitis” of the elbow I.e. Tennis or Golfers’ elbow. Technically they are wrong, and it could be hampering their recovery!!
In actual fact, tendonitis is a very short lived and infrequent tendon condition. What they most likely have is actually TENDINOSIS, or otherwise known as a tendinopathy.
So what’s the big difference you ask? Well, medical terms that end in “itis” usually indicate inflammation and swelling, however in these tendon conditions, no inflammatory cells are present. This then has a direct impact on the way in which we treat the condition. So if you or your friend has tendinosis, taking anti-inflammatory medication is actually having no effect, and you may as well be taking Smarties instead…
If its not inflammation, then what is it exactly?
Without getting too technical, the substance that makes up tendons (collagen) is in a big tangled mess instead of a nice, neat and tight parallel bundles of fibers. There is also increased fluid around the fibers and lots of small, poor quality blood vessels. This can occur in various tendons, but the most commonly affected are those of the elbow (Golfers’ and Tennis Elbow), knee (Jumper’s knee), hip and ankle (Achilles Tendinosis).


So if you shouldn’t take anti-inflammatories, what should you do?
Tendinosis is usually as a result of repeated OVERloading of the tendon and therefore the CAUSE of your problem needs to be addressed. It could be as simple as a lack of rotation at the shoulder that could be causing your tennis elbow, or over-pronation at your ankle causing Achilles tendinopathy. Your physio should evaluate all likely factors and address these to prevent re-occurrence of your injury.
Where previously we were concerned not to inflame the tendon, treatment now focuses on actually CAUSING an inflammatory reaction, thus increasing blood supply and stimulating healing. Although painful, eccentric loading exercises are the “gold standard” of treatment to improve these conditions.
Nitric oxide donor patches and Shock wave therapy have some evidence to suggest they work, and a relatively new technique known as PRP (platelet rich plasma) injections (a topic we will discuss in future posts) are showing positive short term results at reducing pain and improving function.
I would highly recommend wearing a counterforce brace or getting strapped, as this will reducing the mechanical load on the tendon and alleviate pain.
One last thing you need to know. Tendon injuries usually take a long time to heal, especially if you’ve had it for months, so be prepared for some rehab and don’t wait till your pain is excruciating before you seek medical advice.
BY: Riccardo Vaccaro
Ankle injuries / Elbow injuries / Knee injuries / Lower Limb injuries / Shoulder injuries / Upper Limb injuries