
Lateral knee pain (pain felt on the outside of the knee) is a common problem especially among long distance runners and cyclists.
The most common cause of lateral knee pain is probably iliotibial band friction syndrome (ITBFS). Other causes include lateral meniscus abnormalities, patellofemoral syndrome, biceps femoris tendinopathy (one of the hamstring muscles) and superior tibiofibular sprain. In some cases the pain could even be referring from the lumbar spine.
With so many possible causes of lateral knee pain, it is vital to make the correct diagnosis by
a) looking at the mechanism of injury – in other words how you hurt yourself
b) looking at the activity that brings on the pain
c) having specific tests done by your physiotherapist
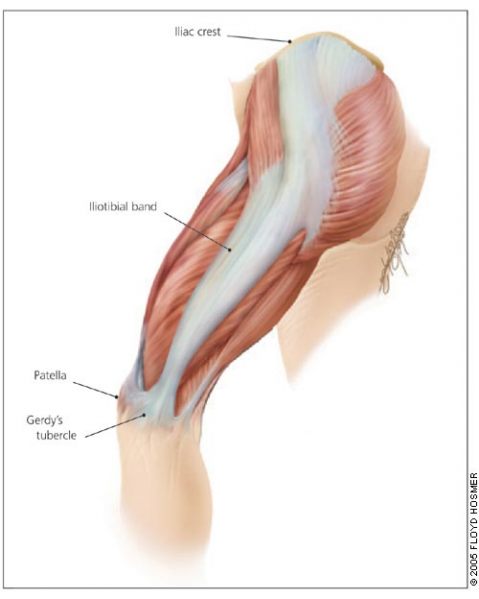
Your Iliotibial band (ITB) is a lateral thickening of the fascia surrounding your thigh. Proximally at the hip the tensor fascia lata muscle inserts into the ITB, as does a portion of the gluteus maximus muscle. Distally the ITB inserts onto the patella and tibia. Thus you can see by its attachments that it plays a role in lateral stability both at the knee and the hip joints.
The ITB has many functions
- Stabilising the pelvis in stance
- Flexion (bending), abducting (moving to the side away from the body) and medial rotation (turning inwards) of the hip
- Stabilising the knee in extension (when its straight)
- Lateral rotation (turning outwards) of the tibia on the femur

Iliotibial band friction syndrome (ITBFS) is an overuse injury presenting as lateral knee pain that is exacerbated by sporting activity. Tenderness is elicited over the lateral femoral epicondyle which is 2-3 cm above the lateral joint line of the knee. The pain often develops at the same time or distance during the aggravating activity. A change in training methods or shoes, longer training and downhill running are often aggravating factors.
Obers test (which would be done by your physiotherapist) would reveal ITB tightness and quite possibly the patient would have tightness and shortening of the tensor fascia lata and gluteus maximus musles, which as discussed earlier, are attached to the ITB.
Treatment with ice and electrotherapy or corticosteroid injection should not only be focused locally on the lateral knee but foot and hip biomechanics should be looked at for more favourable long term results. It has been shown that runners with ITBFS can have significantly weak hip abductors in the affected limb, so focusing on correcting the underlying weakness and fatigability in these muscles is quite important. Myofascial release of the ITB, tensor fascia lata and gluteal muscles as well stretching these muscles is very beneficial. Dry needling and use of a foam roller may also be recommended.
The last resort – if all conservative management fails – is surgery. But before you decided to go under the knife visit your physiotherapist and see if they can’t provide a solution that works for you.
Andrew@PhysioPRO
BY:
Knee injuries, Lower Limb injuries