

Shoes in Sport
Of late, many a client has passed through the door with injuries stemming from incorrect training shoes. Conditions such as: Shin splints, plantar fasciitis, tendinopathies, stress fractures and overuse syndromes may be as a result of the this…
Shoes play and important role in our lives as we wear them most of the time is our daily activities. But how do I know what the right shoe is for my sport?
This is a quick go-to when having a look at which shoe is best suited for you.
Firstly you need to purchase a shoe that is in line with the activity you are performing.
Walking shoes: lightweight, with extra shock absorption in the heel and under the ball of the foot to decrease heel pain and burning/tenderness in the ball of the foot. Walking shoes are more rigid in the frontal area of the shoe for toe roll off. If you feel that you need more even weight distribution, a smoother transition from heel-to-toe and less force over the foot, look for a shoe that has a slightly more rounded sole.
Running shoes: have good overall shock absorption, and heel control. Check your running style first, as a heel-striker requires different shoes to a fore-foot/mid-foot striker!
Aerobic conditioning shoes: lightweight with extra shock absorption in the ball of the foot to prevent foot fatigue.
Tennis and netball shoes: give upper support with quick transferring of weight and side to side movements and a flexible sole for quick changes of direction. When playing on soft surfaces look for a softer sole shoe, and vice versa with a hard surface.
Basketball shoes: have a stiff, thick sole for more stability whilst on court. The high top gives extra ankle support but won’t prevent the risk of ankle injuries.
Cross training shoes: a combination of many features and therefore help you participate in more than one sport, without having to purchase more than one pair of shoes. It will be flexible in the forefoot for running and have lateral control for aerobics and court activities. Obviously, because they are the “jack of all trades” when it comes to functionality, they are not particularly good at any one specific component. For exmple, a cross training shoe shouldnt be worn to run more than 10km. Rather get a dedicated running shoe for that purpose.

How to go about choosing the correct shoe.
-Like clothes- different brands fit differently, so don’t take it for granted that if in the one brand you are a size 7 you would be the same in the next brand.
-Measure both feet when they are at their largest- usually after exercise or at the end of the day. Remember one foot may be larger than the other.
-Use the same type of sock that you would usually use in your activity of preference.
-Comfort is key- the shoe should mimic the shape of your foot
-There is an old saying- “the shoe will become flexible/ loosen with time” this is partially true, however when purchasing a shoe, you should not keep this in the back of your mind. The shoe should be comfortable and fit correctly when purchasing it!
-The widest part of your foot should not feel cramped in the shoe, you should be able to wiggle/ move your toes freely
-The part where your toes are in the shoe (toe box) should have enough depth to prevent chafing, or calluses formation
-Stand and ensure that there is about half the width of your finger between the big toe and the second toe.
-Test the shoe, walk around in it, and ensure that it is comfortable with no chafing. Your heel should not slide forwards and backwards either.
 Some extra tips
Some extra tips
If you participate in a particular sport 3 or more times a week, then a sport-specific shoe is advised.
Shoes need to be replaced depending on how often they are used and age. It is recommended that after 300 hours of aerobic activity, or a maximum of 800km have been reached on the shoes, they have run their course and need to be replaced, much like the tyres on your vehicle. Rubber degrades with age, so a shoe that’s more than 5 years old, regardless of mileage/hours still needs replacing!
These are just a few pointers in helping you find the right fit for your foot. So the next time you head out to upgrade your footwear to what your feet deserve, stop and think before you just choose a brand and type of shoe because of its aesthetic appearance. Choose FUNCTION over FASHION!
Happy shoe shopping!
Amy@physiopro
BY:
Ankle injuries / Foot injuries / General Health/Fitness

Acute injuries- RICE or MEAT?
Things are constantly evolving in the world of sports medicine. With a better understanding of how the human body works, comes an ever changing understanding of how best to treat it. One such notion which needs to be challenged is the age old acronym of R.I.C.E (Rest, Ice, Compress, Elevate) used for the management of acute injuries.

The “Rest” part of this strategy may in fact cause delayed healing and muscle atrophy. Several studies that have compared early PAIN-FREE movement to complete rest have shown decreased healing times and improved pain.
As I stated above, what is quite important is to start moving early on, but specifically without pain. Even some serious injuries/operations should allow for a degree of movement that is pain free.

Another area of uncertainty is the application of “ICE”. Whilst there is evidence that ice causes a numbing effect on tissue (by decreasing the speed and transmission of nerves), thereby reducing pain, the notion that icing decreases the inflammatory response and speeds up healing is being challenged.
Some studies are showing that the application of early ice (for 20 minutes in the acute stage of an injury) may in fact reduce the healing potential of tissue, and cause longer term negative effects on the healing collagen. So if your intention is to reduce pain, then ice may be appropriate, but if you think you are assisting the body healing process, think again…

What is now being suggested is a new acronym – M.E.A.T
MOVEMENT – as discussed earlier, must be pain-free
EXERCISE – the correct exercises done early on have been shown to reduce muscle wasting and improve outcomes
ANALGESICS – used to control acute pain, but be careful not to “mask” the pain so you can go back to activity too quickly. Again, avoid anti-inflammatories at first.
TREATMENT – from a Physiotherapist or other sports medicine practitioner. We can use other modalities to improve circulation and assist healing.
The Editor in Chief of The Physician and Sports Medicine Journal was quoted as saying,”Do you honestly believe that your body’s natural inflammatory response is a mistake?” I’ve said it in my article on anti-inflammatories, the first stage of healing is INFLAMMATION, but it seems we have all been hell-bent on trying to stop this.
It would appear that the more we learn about how to heal the human body, the more we realise it does a pretty good job, all on its own!
Ric@PhysioPRO
BY: Riccardo Vaccaro
Ankle injuries / General Health/Fitness / Knee injuries

Lower Back Pain
Lower Back Pain…Where is it coming from?
Lower back pain is a common injury seen at my practice, both in the sporting and non-sporting population. There are multiple pain producing tissues of lower back pain (muscles, facet joints, ligaments, fascia etc) however, two of the most commonly affected tissues are the disc and nerve. This short article should give you an idea of the difference in symptoms between the two structures.
What is the disc?
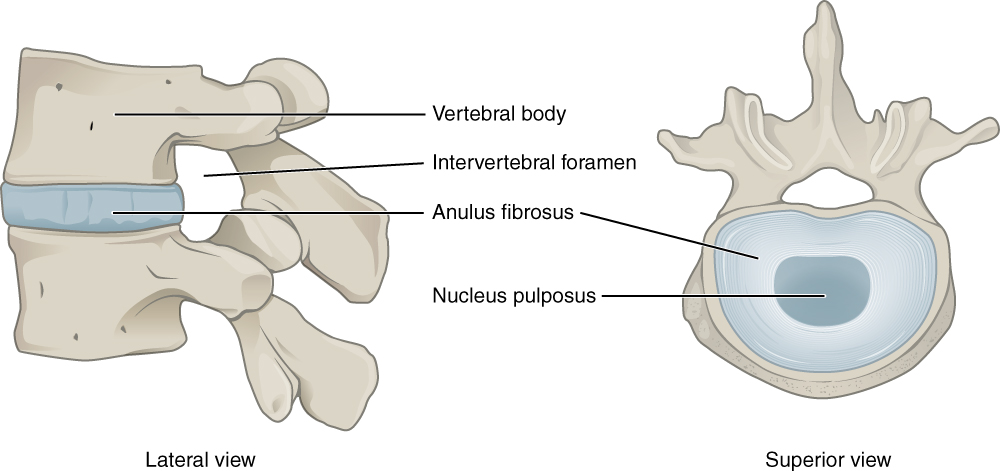
The Intervertebral Disc, is made up of two different tissues…On the outside, we have a thick, tough ring called the Anulous Fibrosus, and on the inside, we have a “jelly-like” material called the Nucleus Pulposus. The disc sits between two vertebral bodies and is not a true “joint”, but acts as more of a shock absorber and allows for one vertebra to move on another. I often tell my patients to imagine a thick layer of jam between two pieces of hard toast. If you squash the toast on one side, the jam gets pushed out the opposite side. For example, when you bend forwards, the jelly inside gets squashed and moves backwards, allowing the two vertebra to move, but not “collapse”.
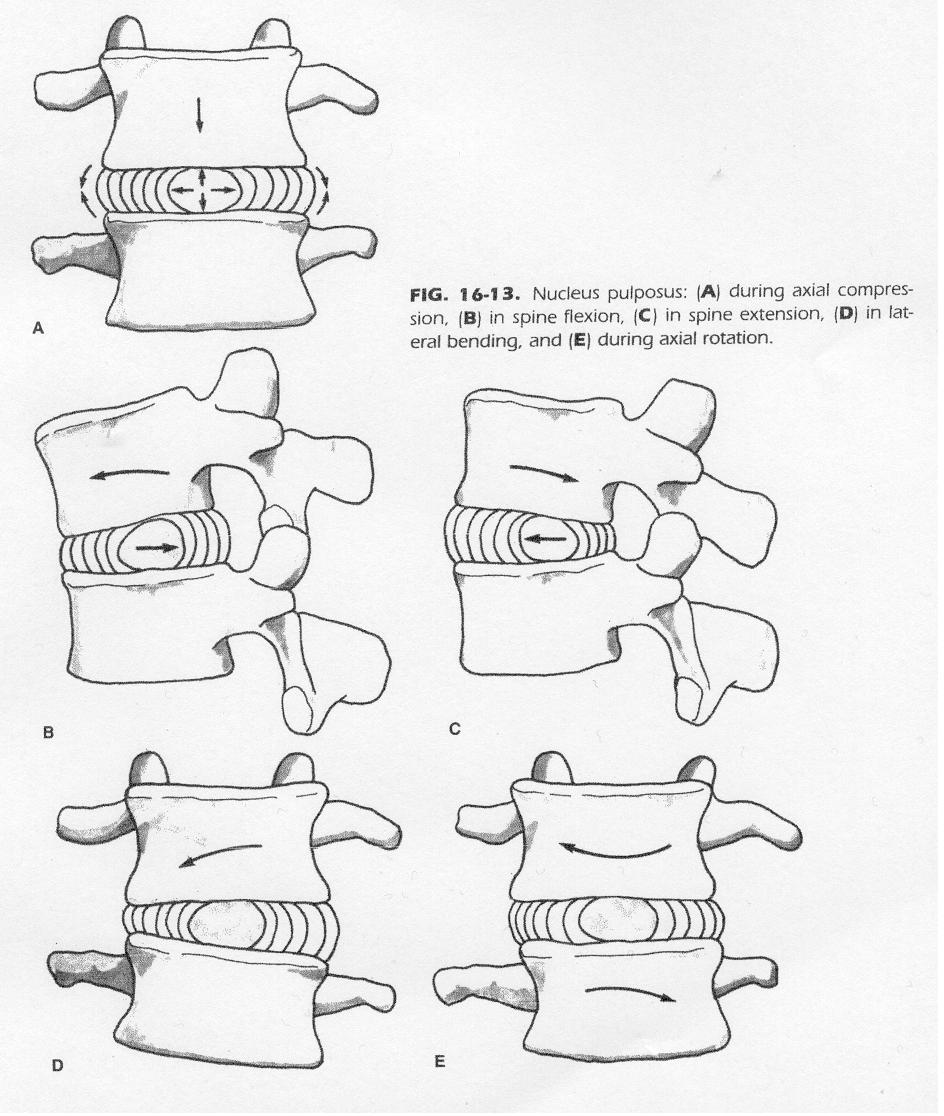
The problem occurs when we put too much loading through the disc, and then force the jelly in a certain direction. A typical example of this is when you bend over to move a heavy box and then you are unable to stand up straight due to the pain in your lower back. The position of the jelly combined with the added weight of the box causes the jelly to be forced backwards and it pushes into the outer ring (see images 1 and 2 below).
This is referred to as a DISC BULGE and can be compounded by a small amount of wear-and-tear of the outer ring (small tears and cracks with ageing). Symptoms of a disc bulge include a broad “band” of pain across the lower back (and sometimes into the buttock) as well as sharp pain with changing positions (sit to stand). Coughing and sneezing are often painful (due to the increase in abdominal pressure, pushing the disc material out further). Usually these disc bulges heal well with physiotherapy techniques (we try to gently squeeze the damaged tissue back in) and anti-inflammatories, and depending on the extent of the damage, can take anywhere from a few days to a few weeks to heal…

If the injury is more severe, we speak of a DISC HERNIATION (Image 3- it has now broken through the outer ring) OR DISC SEQUESTRATION (image 4- part of the jelly has “broken away”). At this point, the inflamed disc and its material often starts to push on the nerve exiting the spine, and now we also have NERVE ROOT IMPINGEMENT.
This is usually accompanied by pain, numbness, weakness and pins/needles of the affected nerve root (pain usually radiates down a part of/or the whole leg), and the pain in the leg usually outweighs the pain in the lower back. These injuries take longer to heal and conservative therapy does have a high rate of recovery, however surgery is sometimes needed.
A nerve can also get trapped where it exits the spine through a little opening called the foramen. Generally this happens in older patients with arthritic degeneration, where the opening becomes narrower due to extra bone formation, enlarged joints and narrowed discs. This produces similar symptoms of pain, numbness and pins/needles but generally, the symptoms gradually appear and get worse with time.

Hopefully this helps you have a better understanding of whats going on in your back.
Ric@Physiopro
BY: Riccardo Vaccaro
Back injuries

The DRUG called Exercise
The wonder drug called… exercise!
Imagine there was a drug you could take that did the following:
- Reduce heart disease by 40%
- Reduce your risk of stroke by 27%
- Decreased diabetes by 50%
- Decreases high blood pressure by 50%
- Lowers deaths and the risk of recurrent breast cancer by 50%, colon cancer by 60%
- Lowers the risk of Alzheimer’s disease by 33%
- Treat depression as effectively as Prozac or other behavioral therapies
Unfortunately there is no pill that can do all these (wishful thinking), but there is a drug out there that can, and it’s called Exercise!!
I recently attended a course by the “Exercise is Medicine South Africa” institute to discuss this very topic of EXERCISE being prescribed as a MEDICINE to all people. It’s part of a global initiative of the American College of Sports Medicine to promote exercise in a safe and effective way.
As with most of the population, most of my patients are aware of the importance of exercise. Those that don’t exercise regularly will always sheepishly admit that they know they should be exercising, but usually blame a lack of time or tiredness as their reason for not doing so.

Here are a few interesting things I picked up from this course:
- Not exercising for ONE day has the same health detriments as smoking THREE cigarettes!!!
As a non-smoker who chooses not to smoke due to the health implications, this came as a big surprise to me and puts into perspective just how damaging it is to be physically inactive.
- Its better to be FAT-AND-FIT than SKINNY-AND-UNFIT
Thats right! Just because you are not overweight doesn’t mean you are healthy.
- If you are not doing at least 150 minutes of exercise per week, you are considered high risk for developing a variety of health issues!!
That basically boils down to getting 30 minutes of exercise for 5 days per week. Less than that and you chances of mortality are more than someone who is obese, or smokes, or has diabetes.
- Being physically active during the day does not count as EXERCISE.
A lot of people believe that they get enough “exercise” by being on their feet all day or climbing a few flights of stairs during their day. The truth is, if your heart rate is not reaching between 50-70% of its maximum capacity for a minimum of 30 minutes (continuously) per day, you can’t say you are exercising.
Work that out quickly for yourself- take 220 and minus your age to get a rough idea of your Heart Rate (HR) max.
Then take your number, and multiply it by 0.5 to get 50% and 0.7 to get 70%.
So for a 35 year old that would be 220-35=185
185X0.5 =92.5 185X0.7=129.5
So this guy or girl would need to have their HR at between 92.5 and 129.5 beats per minute for 30 minutes a day.
On average, a brisk walk would get you into this target heart rate but as with all DRUGS, there are certain risk factors (especially for people who already have pre-existing medical conditions) so this is where Exercise is Medicine South Africa are working with health professionals in order to safely and efficiently prescribe exercise to individuals.
After an initial screening procedure, you would be grouped into either low, moderate or high risk, and your exercise program specifically tailored to suit your risk and needs.
One last thought…
There are 1440 minutes in a day. Can you really not find the time to use 30 of them towards living a longer life???
Ric@PhysioPRO
![]()
BY: Riccardo Vaccaro
General Health/Fitness

Exercising for Knee pain
In May 2012 I wrote an article on “The risk factors in knee pain”. In this article I discussed a study which showed the relevant risk factors in developing ANTERIOR knee pain, or otherwise known as Patello-Femoral Pain Syndrome (PFPS). You can read the article by clicking HERE.
In this study, one of the five risk factors that were found to be associated with PFPS, was “STRENGTH”, specifically that of the Quadriceps muscles which straighten your knee. Some of the advice then given was to strengthen your quadricep muscle through exercises such as squats and resisted knee extension.
Now, in a more recent study which examined the amount of strain placed on the Patello-femoral joint (knee-cap) during different exercises (squats and knee extension), researchers were able to conclude that there are “safe” ranges of motion during these exercises as well as “unsafe” ranges, which would either place a little or a lot of strain on the Patello-femoral joint.
: 
Results:
What the above image demonstrates is that during a squat movement, the “safe” range of motion is between 0 and 45 degrees of knee bending, and the “unsafe” zone from 45 to 90 degrees of bend. So when performing a squat to strengthen the quadricep muscle in PFPS, ONLY GO HALF WAY DOWN!
However, when performing a seated knee extension exercise, the “safe zone” is from 45 to 90 degrees, and the “unsafe zone”, 0 to 45 degrees of bend. So when performing a resisted leg extension exercise, ONLY GO HALF WAY UP!
By training in the “safe” zones for both of these types of exercises, you can strengthen your quadriceps muscles and at the same time, avoid feeling knee pain. If you are already experiencing pain under your knee cap, always consult your Physio prior to starting these exercises. Once you can do these exercises pain free, your Physio will progress them accordingly.
Ric@PhysioPRO
Article by Powers et al, titled “Patellofemoral Joint Stress During Weight-Bearing and Non–Weight-Bearing Quadriceps Exercises,” J Orthop Sports Phys Ther 2014;44(5):320-327. Epub 27 March 2014.doi:10.2519/jospt.2014.4936
BY: Riccardo Vaccaro
Knee injuries / Lower Limb injuries

Take this pill-tear that muscle!
So you go to see your doctor because you have the flu. The doctor books you off and prescribes antibiotics. One or two weeks later you start to feel better so you decide to go for a jog, and thats when it happens! Suddenly you hear a loud “crack” and start limping. You’ve TORN your achilles tendon and you weren’t even straining yourself?
This same scenario has happened to many people and its not because they were sick or unfit, its because of the ANTIBIOTIC that was prescribed!!!
A group of Antibiotics called Flouroquinolones are associated with a wide variety of musculoskeletal problems that affect muscle, tendon, bone and cartilage. They are commonly used to treat a variety of urinary tract, digestive, respiratory and skin infections amongst others. In the USA, this class of antibiotic is THE most prescribed type to adults, even though since as early as 1983 it was known that this drug was toxic to musculoskeletal tissue. Symptoms have been known to occur as early as 2 hours after the initial dosage and as late as 6 months after!!
In one study of 42 patients who developed Tendon related problems, 76% experienced tendinopathy (sick tendons) and the other 24% had complete ruptures of the tendon. Muscle symptoms range from mild muscular pain to a very serious and life threatening condition known as Rhabdomyolysis. Bone problems are less conclusive in humans, but in animal studies, it has been shown to slow down or even stop a bone from repairing itself.
What they have discover in more recent times is that there are factors which make you more at risk of developing these symptoms. These include: increasing age, use of cortisone, playing sport, a previous history of tendon or joint problems, magnesium deficiency and diabetes to name but a few.
So what should you do or how can this be avoided?
Not to discredit any Doctor or other health professional, but if you are being prescribed an anti-biotic, check with them that this will be safe to use, especially if you are a physically active person. I had a patient recently that developed general muscle ache, along with severe elbow pain for no apparent reason. She had all the symptoms of someone that had trained heavily the past few days, which she hadn’t. She also had Tennis elbow symptoms and it turned out she was prescribed a Flouroquinolone by her dentist for a tooth infection the week before…
So your doctor should get a thorough history of your previous musculoskeletal problems, find out about your activity levels, ask about associated risk factors and advise you to stop the drug immediately if it is causing any symptoms.
If you are an Athlete, you should definitely not be using this class of antibiotic unless there is no available alternative drug. If you are presently taking this drug, or have used it in the past 6 months, reduce your training intensity, avoid ballistic movements and be aware of any development of symptoms.
Ric@PhysioPRO
Full article by Hall et al. Published in the American Academy of Physical Medicine and Rehabilitation, Vol 3. 132-142, Feb 2011.
BY: Riccardo Vaccaro
General Health/Fitness

Modified Shoulder Stretches
Sometimes just by modifying the position or way you perform a stretch slightly, you can have much better results and outcomes. So when I came across an article about two modified shoulder stretches, I just had to share it with all of you.
Two of the most commonly used shoulder stretches to increase the flexibility of the posterior soft tissues are the cross-body and sleeper stretch exercises. But, based on the inability to stabilize the shoulder blade and control glenohumeral joint rotation with the cross-body stretch and the potential for subacromial impingement with the sleeper stretch, it has been recommend that modifications to both of these commonly performed stretches be made.
The modified sleeper stretch is performed with the athlete in a sidelying position, trunk rolled posteriorly 20° to 30°, and shoulder elevated to 90°. In this position, the athlete passively pushes his forearm down towards the bed using the opposite arm, a towel may also be placed under the arm of the stretched limb. This modified sleeper stretch position puts the posterior structures of the shoulder under more tension thus making it more effective.
 The cross-body stretch is often performed with the athlete in an upright standing position, using the opposite hand to horizontally adduct the targeted shoulder (pull your arm across your body).
The cross-body stretch is often performed with the athlete in an upright standing position, using the opposite hand to horizontally adduct the targeted shoulder (pull your arm across your body).
This method has the disadvantage of not providing stability to your shoulder blade and allows excessive external rotation of your shoulder. Due to this optimal stretch of the posterior shoulder is not achieved. Therefore, to better stabilize the shoulder blade, it has been suggested that the athlete be in a sidelying position, and, to restrict external rotation of the shoulder,the athlete should align the forearms together with the opposite forearm on top.

Well I hope these little adjustments to your stretching techniques yield large results.
Andrew@PhysioPRO
Reference: Journal of Orthopaedic & Sports Physical Therapy, 2013, Volume: 43 Issue: 12 Pages: 891-894
BY:
Shoulder injuries / Upper Limb injuries

Glorious Gluteus Muscles!
Back in 2011 I wrote an article called “How your BUM controls your BODY”. In the article I explained why the gluteus muscles are such an important muscle to train because it directly affected your ankles, knees and hips. If you haven’t already read it, then I suggest you go read it by clicking here.
In about 90% of lower leg injuries, I find that these gluteus muscle needs strengthening, so its crucial if you have any of those conditions mentioned in the previous article. In the article I only showed one exercise to do that targeted that gluteus muscle. Today I want to give you some more so you can really work it.
Advanced Clam


The starting position for this exercise is much the same as for the original Clam shell exercise (lying on your side,knees bent and heels touching). Place your forearm on the floor and then “push” your bottom knee into the floor, forcing your body to lift up off the floor-similar to a side plank. Now move the top knee up and down, but keep the heels touching.
The difference here is that you are training BOTH bum muscles at the same time. The bottom leg’s bum muscle is having to hold you up whilst keeping static (isometric) whilst the top leg’s bum muscle is moving the top leg (concentric). Trust me, it’s a real killer and you should feel the burn in your bum, right behind your hip. Once you can do 3 sets of 15 reps, then try adding an elastic band around your knees. An added advantage of this exercise is that is also trains your core at the same time!

This one looks easy but don’t be fooled… Stand with one leg over the edge of a step. Now keeping both knees LOCKED OUT STRAIGHT, lower your one leg by dropping your pelvis down on that side (keep those knees straight!). Now lift that leg as high up as you can and repeat. You want to concentrate on slowly lowering the leg (eccentric movement), and you should feel a burn in the gluteus muscle of the leg that you are standing on. Again, do 3sets of 10-15, but the slower you go the better.
So there you have it, two more exercises to add to your prevention program! And to all my CrossFit Athletes, this WILL help with your squat form! Tight buns
Ric@PhysioPRO
BY: Riccardo Vaccaro
Foot injuries / Hip injuries / Knee injuries / Lower Limb injuries

Osgood-Schlatter lesion
Anterior knee pain is a common complaint among sportsmen. One of the main causes of anterior knee pain in younger athletes is a condition known as Osgood-Schlatter lesion.
This condition is extremely common in teenage boys with a high level of physical activity, generally occurring at the time of a growth spurt. Mainly associated with sports involving a lot of running and jumping e.g. basketball, soccer, gymnastics etc.
 Examination reveals tenderness and pain over the tibial tuberosity (a small outgrowth on the shin bone where the patellar tendon attaches), with associated tightness of the quadriceps muscle. Excessive subtalar pronation (flat feet) may predispose the adolescent to the development of this condition.
Examination reveals tenderness and pain over the tibial tuberosity (a small outgrowth on the shin bone where the patellar tendon attaches), with associated tightness of the quadriceps muscle. Excessive subtalar pronation (flat feet) may predispose the adolescent to the development of this condition.
The pain is mostly aggravated by exercise and thus the management of the condition requires the athlete to modify their activity levels i.e. the less activity they do, the less pain they will have. Osgood-Schlatter lesion is a self-limiting condition, which means with time it will resolve by itself but may take up to 2 years. This can be very frustrating for the athlete and parents especially if they do not understand the nature of the condition. In the long term the athlete may develop a thickening and prominence of the tibial tubercle which will present as a bump on their shin bone just below the knee.
When the athlete is suffering from pain the symptomatic management includes icing the region, electrotherapy, massaging and releasing the quadriceps muscle, stretching as well as correcting any subtalar pronation if present.
So if you are suffering from this condition head to your local physiotherapist for advise and treatment.
Andrew@PhysioPRO
BY:
Knee injuries / Lower Limb injuries